
AI & IBD – Opportunities and Directions
AI & IBD – Opportunities and Directions
May 26, 2026
Issue 05
Mentoring in IBD is an innovative and successful educational program for Canadian gastroenterologists that includes an annual national meeting, regional satellites in both official languages, www.mentoringinibd.com, an educational newsletter series, and regular electronic communications answering key clinical questions with new research. This issue is based on the presentation made by Dr. Peter Rossos, at the 26th annual national meeting, Mentoring in IBD XXVI: The Master Class, held in Toronto on November 14, 2025.
Introduction
Artificial intelligence (AI) is not a recent innovation, but rather a concept that has been developing since the 1950s.1 More recently, generative AI has emerged as a defining advancement, enabling systems not only to analyze information but also to create new content based on user prompts and existing data. The objectives of this presentation were to develop a shared understanding of what defines AI, explore benefits and risks of AI in healthcare, discuss how AI can support inflammatory bowel disease (IBD) care and how to effectively integrate AI into clinical practice.
AI Integration in Healthcare
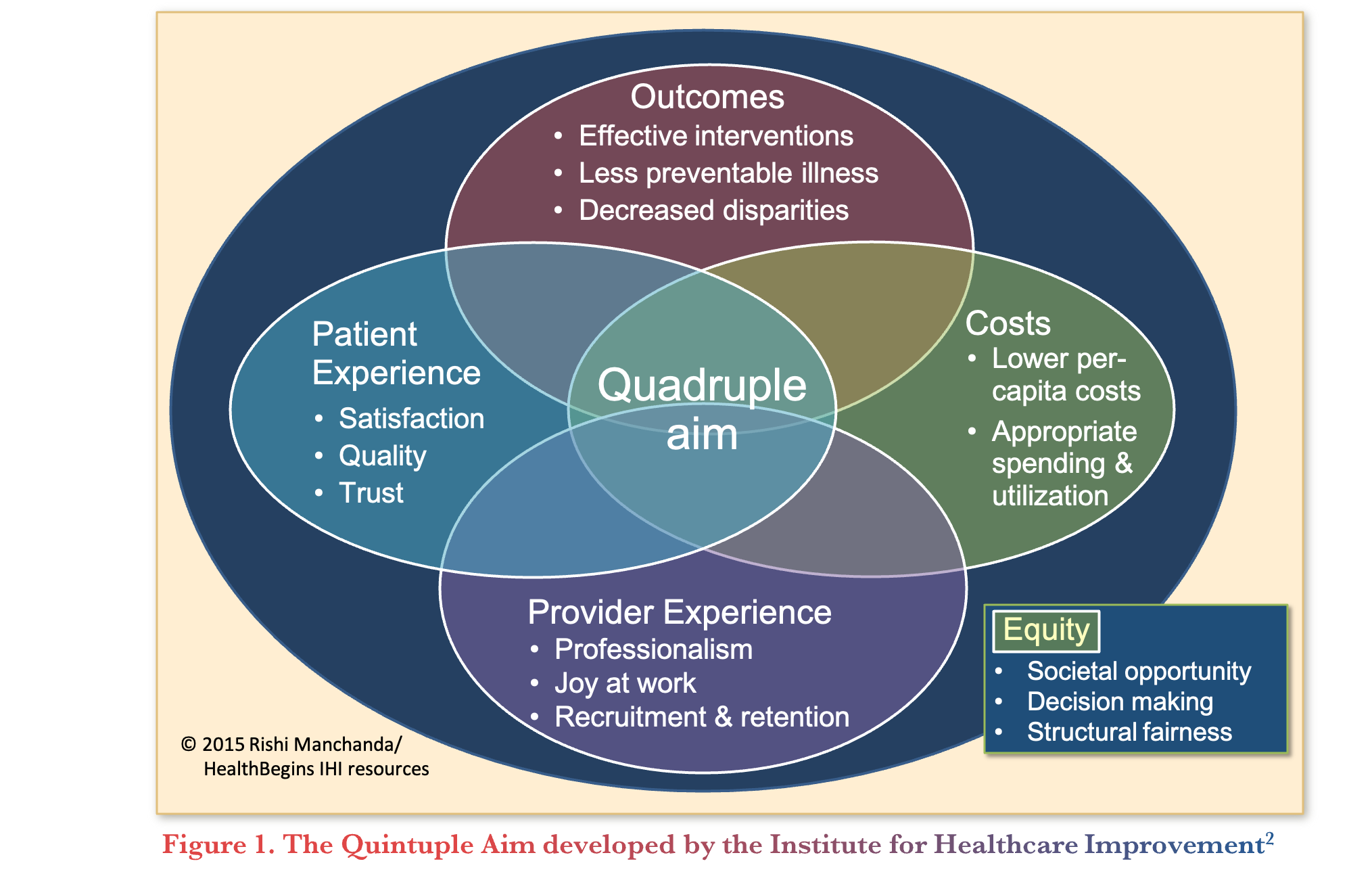
AI is increasingly shaping the future of healthcare, representing a fundamental shift in how technology can be used in clinical environments. The Institute for Healthcare Improvement developed the Quintuple Aim (Figure 1), a framework to guide health system transformation, based on five components: improving patient experience, enhancing population health, reducing costs, supporting provider well-being, and advancing health equity.2 These elements are interdependent, with progress in one area often influencing outcomes in the others. AI has the potential to support improvements across the five components but can also introduce risks if not implemented carefully.
Applications of AI in Healthcare and IBD Care
The AI taskforce from the American Society for Gastrointestinal Endoscopy published core competencies for gastroenterologists to familiarize themselves with understanding basic AI concepts, recognizing ethical and societal implications, evaluating evidence, and interpreting decision support tools.3 These competencies are particularly relevant given the expanding range of AI applications in clinical practice.
AI is already being used in several areas of clinical practice. These include AI scribes, clinical decision support, workflow optimization, coding and billing, remote patient monitoring, and patient engagement. Additional areas of development include endoscopy and diagnostic imaging, histologic reporting and image analysis, as well as genomics, biomarkers, and drug discovery.4
A recent publication by Ahmed and colleagues5 explored how AI is used in IBD care. Specifically, AI was described as having the potential to replicate expert judgment and address possible clinician disagreements, subjectivity and bias. For example, AI can support more objective endoscopic scoring, as current scoring systems are based on qualitative judgments that are influenced by clinician experience and subject to bias and variability. The authors further added that AI can create more detailed and comprehensive objective disease measurements and perhaps identify findings not visible to the human eye.5
Endoscopy and Image Analysis
One of the most advanced applications of AI in IBD is in endoscopy and image analysis. For example, AI-assisted tools are being used to measure quality metrics such as cecal intubation rates, bowel preparation scores, and the percentage of mucosa visualized. These features are expected to become standard in future endoscopy systems, if not already integrated.
Computer vision represents an important and evolving area, allowing systems to identify features that may not be visible to clinicians. This includes integration of different imaging modalities, development of new disease scoring systems, and correlation with histology and outcomes.6
Additional developments include heat maps, vascular assessments, and automated reporting systems, as well as the ability to track procedural metrics, and generate performance reports. AI also enables the integration of multiple data sources, including clinical data, imaging, histology, biomarkers, and patient monitoring to support predictive modeling and more personalized approaches to care.6
Wearable Devices
Commonly used wearable devices like fitness rings and watches can provide physiological signals such as heart rate, some of which have been associated with IBD activity. In a pilot study, physiological data was collected from wearable devices (Apple Watch, Fitbit, and Oura Ring) among participants diagnosed with IBD.7 The fitness trackers identified altered patterns up to 7 weeks prior to inflammatory and symptomatic flares. While AI was not directly applied in this study, these findings highlight the growing role of digital health technologies and the potential for AI-driven tools to use such data to predict disease flares before symptoms or biomarker changes become apparent.7
Administrative Efficiency and Patient Communication
AI scribes have been shown to significantly reduce administrative workload among primary care physicians (PCP) and specialists. An initiative supporting AI scribe integration for PCP across Canada has resulted in high levels of satisfaction among clinicians. Almost all PCP (93%) felt more present with patients during visits, 89% experienced reduced administrative workload, and 85% reported lower cognitive burden.8 Similarly, an Ontario-specific initiative found that AI scribes resulted in family physicians spending 70% less time on paperwork and saving ~3-4 hours per week.9
In larger settings like hospital-based environments, generative AI is being used for tasks such as drafting texts, generating summaries, automating tasks, and translating content. These capabilities are increasingly being integrated into electronic health record systems rather than used as standalone tools, supporting both in-person and asynchronous care.
AI can also support patient scheduling, reminders, and communication. As an example, Ochsner Health launched a pilot program that uses AI to draft messages to patients to support more timely responses.10 All messages were reviewed by the physicians to ensure accuracy prior to sending. The results showed that satisfaction was consistently higher with AI-generated responses than with clinician responses. Furthermore, findings suggest that the brevity of responses from clinicians could be a factor that lowers satisfaction, whereas AI responses tended to be longer and more comprehensive.11 However, to optimally integrating AI into patient–clinician communication, patients must be recognized as essential contributors for the development and implementation of the AI tools.
AI Models and Accessibility
In parallel to different applications of AI in healthcare, the types of AI models are also evolving. AI models can be broadly categorized based on how they are developed and deployed, including proprietary systems and open-source models. Through exploring how AI is currently used and may be used in IBD care, several questions remain about how AI models will be trained, how bias and discrimination will be avoided, who will decide which models are used, and whether access will be equitable in IBD care. Thus, the real-world use of AI requires extensive validation in a diverse number of clinical settings.5
A study by Buckley and colleagues12 found that an open-source large language model (Llama 3.1), which can be downloaded and run locally within a healthcare system, performed comparably to GPT-4, a proprietary model accessed through external platforms, in diagnosing complex medical cases based on clinical records from the New England Journal of Medicine. These findings suggest that high-performing AI models may no longer be limited to company-controlled systems. As a result, there is growing potential for local deployment of AI within healthcare organizations, which could reduce costs and address privacy concerns. Overall, this reflects a broader trend toward making AI more accessible and easier to integrate into clinical workflows.
Risks and Limitations of AI
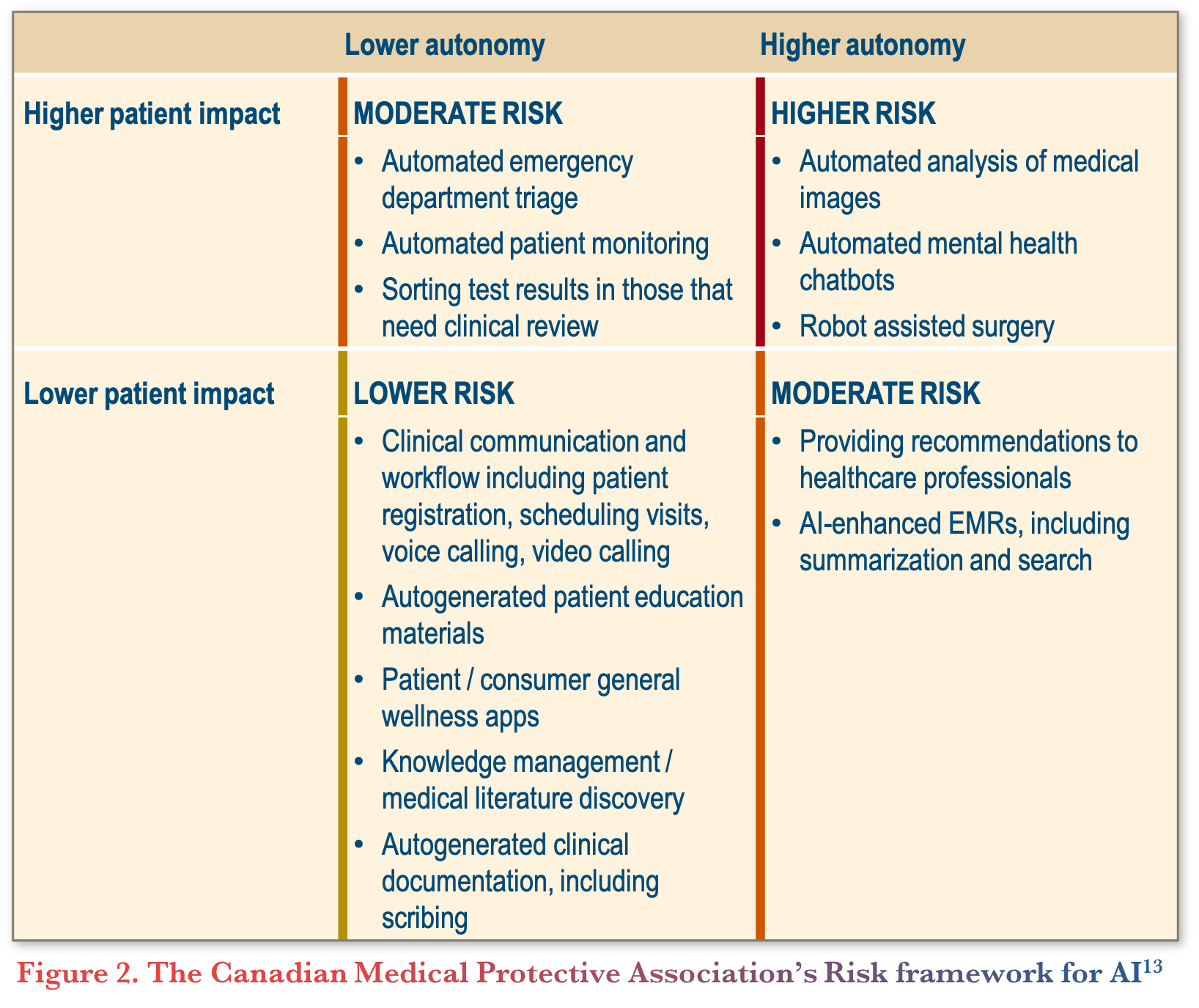
A risk-based framework categorizes AI applications according to their level of potential impact (Figure 2). Lower-risk applications include AI scribes and patient communication tools, while higher-risk applications include automated image analysis, mental health tools, and robotic surgery.13
In addition to application-specific risks, several broader concerns have been identified with the use of generative AI in clinical practice such as model drift and hallucinations. Model drift refers to the gradual decline in an AI model’s performance over time as clinical practices, patient populations, or data patterns change, leading to outputs that may no longer be accurate or reliable. Hallucinations refer to instances where AI scribes generate information that appears plausible but is incorrect or not based on the actual conversations. Other possible risks include the potential for increased workload expectations for physicians, and the cost and the environmental impact of such technologies.
Human Decision-Making and Skills vs. AI
While evidence suggests that AI may outperform clinicians in certain scenarios, outcomes may worsen when its recommendations are overridden without appropriate consideration. This highlights the need to understand when to rely on AI, when to apply clinical judgment, and when to combine both approaches. The path forward may involve physicians working with AI for the optimal partnership model.14 Furthermore, regulatory oversight remains limited for some AI tools, particularly those used for documentation and to support clinical decision-making.15
There are additional concerns regarding loss of clinical skills, particularly if clinicians rely heavily on AI-assisted tools. Training programs may need to address this by ensuring continued exposure to non-AI-assisted practice. At the same time, human skills remain essential, such as communication, compassion, understanding patient context, anticipating needs, and adaptability.
Conclusions
AI is particularly relevant in IBD due to the complexity and volume of data involved in disease management. It has the potential to improve access to care and increase the time available for clinicians and patients to focus on meaningful interactions. At the same time, careful attention must be given to safety, effectiveness, and ethical considerations. Clinicians are encouraged to develop familiarity with AI tools, use them in practice, and remain aware of both their benefits and limitations.
Survey
Question 1: Current Engagement
How is AI being used in your current clinical practice?
Commentary
- Most gastroenterologists use AI for researching clinical questions with tools such as ChatGPT.
- Less common uses of AI include endoscopy, clinic operations, external services such as radiology or pathology, and administrative tasks.
- A primary barrier to AI scribes in practice is data privacy and security requirements within hospital systems.
- Many clinicians are currently experimenting with AI in an informal or exploratory way, rather than integrating it into routine clinical workflow.
Question 2: Current Status
How would you describe your current understanding of AI?
Commentary
- Most gastroenterologists understand the basics of AI but do not feel confident in their depth of knowledge.
Question 3: Future Opportunities
Which areas of gastroenterology practice will significantly change as a consequence of AI?
Commentary
- Gastroenterologists believe that AI is expected to impact multiple areas of practice, including endoscopy, disease prediction and prognosis, practice management, quality metrics, and report generation.
- Although there is a rapid increase in research using AI and for endoscopic image assessments, these developments are not being integrated into clinical practice, raising concerns about the gap between innovation and implementation.
Question 4: Physician Attitudes
Which of the following best describes your attitude to future involvement of AI in the clinical practice of gastroenterology?
Commentary
- The most common response reflected a balanced perspective, where gastroenterologists acknowledge the potential benefits of AI but also expressed concern about its risks.
- For example, AI may enhance disease assessment by detecting subtle, clinically relevant changes beyond traditional scoring systems, but raises concerns regarding unclear reference standards and the potential to identify findings that may not be clinically meaningful.
Question 5: Patient Attitudes
How have your patients integrated AI into their health care?
Commentary
- Patients are using AI for self-diagnosis, research and education, interpretation of results, and seeking health advice.
- Given that patients are already actively engaging with AI tools, clinicians may increasingly encounter patients who come with AI-generated information or perspectives on their care.
References
-
- McCarthy J, Minsky ML, Rochester N, Shannon CE. A proposal for the Dartmouth summer research project on artificial intelligence. 1955.
- Nundy S, Cooper LA, Mate KS. The quintuple aim for health care improvement: a new imperative to advance health equity. JAMA. 2022;327(6):521–2.
- ASGE AI Task Force, Parasa S, Berzin T, et al. Consensus statements on the current landscape of artificial intelligence applications in endoscopy, addressing roadblocks, and advancing artificial intelligence in gastroenterology. Gastrointest Endosc. 2025;101(1):2–9.e1.
- Ahmed M, Stone ML, Stidham RW. Artificial intelligence and IBD: where are we now and where will we be in the future?. Curr Gastroenterol Rep. 2024;26:137–44.
- Gu P, Mendonca O, Carter D, et al. AI-luminating artificial intelligence in inflammatory bowel diseases: a narrative review on the role of AI in endoscopy, histology, and imaging for IBD. Inflamm Bowel Dis. 2024;30(12):2467–85.
- Ahmed S, et al. Artificial intelligence in inflammatory bowel disease. Curr Gastroenterol Rep. 2024;26:137–44.
- Hirten RP, Danieletto M, Sanchez-Mayor M, et al. Physiological data collected from wearable devices identify and predict inflammatory bowel disease flares. Gastroenterology. 2025;168(5):939–51.e5.
- Canada Health Infoway. AI scribe program. Canada Health Infoway. https://www.infoway-inforoute.ca/en/featured-initiatives/ai-scribe-program. Accessed April 8, 2026.
- OntarioMD. Clinical evaluation of artificial intelligence and automation technology to reduce administrative burden in primary care: AI scribe evaluation final report. OntarioMD; July 31, 2024. https://www.ontariomd.ca/documents/ai%20scribe/ai%20scribe%20evaluation_final%20report_vf.pdf. Accessed April 8, 2026.
- Ochsner Health. Ochsner health to integrate generative AI into patient messaging. EurekAlert! September 18, 2023. https://www.eurekalert.org/news-releases/1001842. Accessed April 8, 2026.
- Kim J, Chen ML, Rezaei SJ, et al. Perspectives on artificial intelligence-generated responses to patient messages. JAMA Netw Open. 2024;7(10):e2438535.
- Buckley TA, Crowe B, Abdulnour RE, Rodman A, Manrai AK. Comparison of frontier open-source and proprietary large language models for complex diagnoses. JAMA Health Forum. 2025;6(3):e250040.
- Canadian Medical Protective Association. The medico-legal lens on AI use by Canadian physicians. Canadian Medical Protective Association; September 2024. https://www.cmpa-acpm.ca/en/research-policy/public-policy/the-medico-legal-lens-on-ai-use-by-canadian-physicians. Accessed April 8, 2026.
- Topol E. Why doctors are better than AI at diagnosis—for now. New York Times. December 1, 2024. Accessed April 9, 2026. https://www.nytimes.com/2024/12/01/opinion/ai-doctors-diagnosis.html.
- Goodman KE, Yi PH, Morgan DJ. AI-generated clinical summaries require more than accuracy. JAMA. 2024;331(8):637–8.
Editor-in-Chief
John K. Marshall, MD MSc FRCPC CAGF AGAF
Professor, Department of Medicine
Director, Division of Gastroenterology
McMaster University
Hamilton, ON
Contributing Author
Peter G. Rossos, MD MBA FRCP(C) FACP CAGF
CMIO University Health Network
Professor, Division of Gastroenterology and
Institute of Health Policy, Management and Evaluation (IHPME),
Department of Medicine, University of Toronto
Toronto, ON
Mentoring in IBD Curriculum Steering Committee
Alain Bitton, MD FRCPC, McGill University, Montreal, QC
Karen I. Kroeker, MD MSc FRCPC, University of Alberta, Edmonton, AB
Cynthia Seow, MBBS (Hons) MSc FRACP, University of Calgary, Calgary, AB
Jennifer Stretton, ACNP MN BScN, St. Joseph’s Healthcare, Hamilton, ON
Eytan Wine, MD PhD FRCPC, University of Toronto, Toronto, ON
IBD Dialogue 2026·Volume 22 is made possible by unrestricted educational grants from…
![]()
![]()

![]()
![]()



![]()
![]()
![]()
Published by Kalendar Inc., 7 Haddon Avenue, Scarboro, ON M1N 2K7
© Kalendar Inc. 2026. All rights reserved. None of the contents may be reproduced in any form without prior written permission from the publisher. The opinions expressed in this paper are those of the authors and do not necessarily reflect the opinions or recommendations of the sponsors, the grantor, or the publisher.
.