
What is the role of fecal calprotectin in monitoring in the treat-to-target strategy in IBD?
What is the role of fecal calprotectin in monitoring in the treat-to-target strategy in IBD?
Smita Halder, MD
Volume 2 | Issue 3
Runs 1:35
Fecal calprotectin is an important reliable, simple, inexpensive, and safe biomarker in inflammatory bowel disease (IBD) that can distinguish inflammatory from noninflammatory disease.(1) Fecal calprotectin levels correlate well with both endoscopic and histologic findings.(2–5) This biomarker may therefore have a role in proactive monitoring of patients in remission, and it may reduce the number of endoscopies required. In the treat-to-target strategy, fecal calprotectin is considered an adjunctive biomarker, rather than a treatment target, in measuring treatment response and mucosal healing and predicting relapse.(6) Calprotectin can also support differentiation of IBD from irritable bowel syndrome (IBS).(7)
Fecal calprotectin in diagnosis
An evidence-based pathway using fecal calprotectin testing was developed to assist primary care physicians in diagnosing IBS without referral, increase referral for likely IBD, and enhance patient care.(7) This clinical decision-making support tool improved decision-making, resulted in faster diagnosis with rapid colonoscopy, and provided an increased diagnostic yield after referral than conventional approaches.
Fecal calprotectin in remission
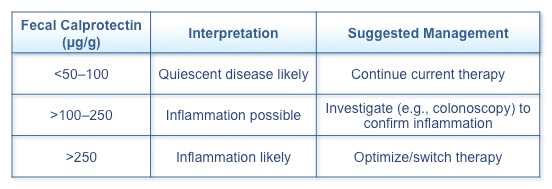
A review of the literature indicates that fecal calprotectin testing of the first morning sample should be used as the standard of care to confirm inflammation when an IBD flare is suspected.(8) Nevertheless, the role of fecal calprotectin in routine monitoring in the treat-to-target strategy has not yet been determined, as additional data are required to define optimal cutoff levels and patients who can benefit the most. Suggested cutoff values and management strategies for adults with IBD have been identified (Table 1).
Table 1. Fecal Calprotectin and Clinical Approaches(8)
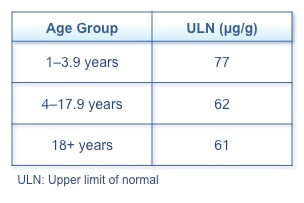
In children, a retrospective study identified reference ranges for the upper limit of normal fecal calprotectin by age group (Table 2).(9) Children between 1 and 3.9 years had higher concentrations of fecal calprotectin than older children and adults, but no significant difference was seen between older children and adults.
Table 2. Fecal Calprotectin Upper Limit of Normal by Age Group(9)
Fecal calprotectin in treat to target
The Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE) program examined potential targets and the evidence supporting them and developed consensus recommendations for treatment targets for ulcerative colitis (UC) and Crohn’s disease (CD).(6) In patients with CD, STRIDE stated that fecal calprotectin may be a useful adjunctive biomarker to measure response to therapy and predict relapse, especially in Crohn’s colitis and after ileocecectomy. In UC, fecal calprotectin correlates well with response to induction and mucosal healing and predicts loss of response to maintenance. Failure of normalization with therapy should prompt additional endoscopic evaluation. In both UC and CD, insufficient evidence exists to recommend treatment optimization based on fecal calprotectin alone. Evidence on the correlation between fecal calprotectin and endoscopy and fecal calprotectin and histology is, however, accumulating.
Fecal calprotectin and endoscopy
As fecal calprotectin levels correlate well with endoscopic findings, routine use of fecal calprotectin for monitoring in the treat-target strategy may significantly reduce the number of endoscopies required.(2) What still needs to be determined is whether this biomarker can replace endoscopic mucosal healing as a treatment target, the optimal time for testing after induction, and whether changes from baseline more accurately reflect response than standard cut-off levels, as these may vary between individual patients.
Point-of-care tests
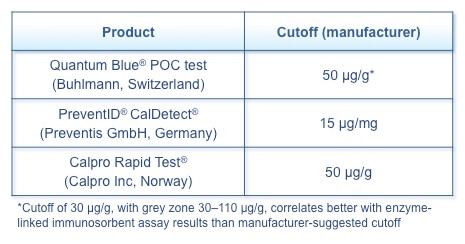
Reliable and accurate point-of-care tests that allow rapid testing in the patient’s home or the clinician’s office increase the accessibility and feasibility of fecal calprotectin testing (Table 3).(2) In endoscopy-proven IBD, the results for both point-of-care tests and standard techniques were similar, although no large comparisons have been performed. Using the first morning fecal sample reduces intertest variability.
Table 3. Fecal Calprotectin Point-of-Care Tests(2)
Fecal calprotectin and histology
Several studies have demonstrated the correlation of fecal calprotectin levels with histologic findings.
A multicentre cohort study evaluated the use of histology as a treatment target and the utility of fecal calprotectin in predicting histologic disease activity.(3) The study included 20 patients with moderately-to-severely active UC who were initiated on infliximab treatment and measured histologic remission at 8 weeks. Histologic remission was seen in 15% and mucosal healing was achieved in 45% at 8 weeks. Fecal calprotectin was correlated with histologic activity at week 8 (area under the curve 94%, P=0.017) and had an excellent positive predictive value (100%, P=0.017).
A 12-month prospective observational study of 70 patients with UC in endoscopic remission assessing the ability of fecal calprotectin and histologic inflammation to predict relapse found that baseline fecal calprotectin >321 mg/kg predicted disease relapse at 6 and 12 months.(4) Although histologic inflammatory activity did not predict relapse, patients with histologic inflammation had significantly higher fecal calprotectin levels than those without histologic inflammation. These results support more frequent follow-up of asymptomatic patients with elevated fecal calprotectin to identify impending relapse.
A study examining the correlation of fecal calprotectin with histologic and endoscopic remission in colonic IBD included 58 patients, 23 with colonic CD and 35 with UC.(5) Low fecal calprotectin (<100 μg/g) was highly correlated with histologic remission in both UC and colonic CD and had the highest sensitivity for clinical and endoscopic remission for both patient groups. Histologic features tend to improve more slowly than clinical and endoscopic status, and the impact of histologic remission on outcomes has yet to be fully defined. Using fecal calprotectin to monitor patients with colonic IBD may decrease the need for endoscopy to differentiate quiescent from active disease and identify patients who require more intensive therapy.
References
- Ben-Horin S, Mao R, Chen M. Optimizing biologic treatment in IBD: objective measures, but when, how and how often? BMC Gastroenterology. 2015;15(178):1–7.
- Kopylov U, Rosenfeld G, Bressler B, et al. Clinical utility of fecal biomarkers for the diagnosis and management of inflammatory bowel disease. Inflamm Bowel Dis. 2014;20:742–56.
- Magro F, Lopes SI, Lopes J, et al. Histological outcomes and predictive value of faecal markers in moderately to severely active ulcerative colitis patients receiving infliximab. J Crohns Colitis. 2016 May 25. pii: jjw112. [Epub ahead of print]
- Theede K, Holck S, Ibsen P, et al. Fecal calprotectin predicts relapse and histological mucosal healing in ulcerative colitis. Inflamm Bowel Dis. 2016;22:1042–8.
- Zittan E, Kelly OB, Kirsch R, et al. Low fecal calprotectin correlates with histological remission and mucosal healing in ulcerative colitis and colonic Crohn’s disease. Inflamm Bowel Dis. 2016;22:623–30.
- Peyrin-Biroulet L, Sandborn W, Sands BE, et al. Selecting therapeutic targets in inflammatory bowel disease (STRIDE): determining therapeutic goals for treat-to-target. Am J Gastroenterol. 2015;110:1324–38.
- Turvill J, O’Connell S, Brooks A, et al. Evaluation of a faecal calprotectin care pathway for use in primary care. Prim Health Care Res Dev. 2016 Feb 22:1–9. [Epub ahead of print]
- Bressler B, Panaccione R, Fedorak RN, et al. Clinicians’ guide to the use of fecal calprotectin to identify and monitor disease activity in inflammatory bowel disease. Can J Gastroenterol Hepatol. 2015;29(7):369–
- Davidson F, Lock RJ. Paediatric reference ranges for faecal calprotectin: a UK study. Ann Clin Biochem. 2016 May 1. pii: 0004563216639335. [Epub ahead of print]
Special Edition IBD Dialogue 2016 Volume 02: Treat-to-Target in IBD is made possible by an unrestricted educational grant from…
![]()