
IBD Mimickers
IBD Mimickers
June 23, 2020
Issue 05
Mentoring in IBD is an innovative and successful educational program for Canadian gastroenterologists that includes an annual national meeting, regional satellites in both official languages, www.mentoringinibd.com, an educational newsletter series, and regular electronic communications answering key clinical questions with new research. This issue is based on the presentation made by the contributing editor, Dr Franck Carbonnel, at the 20th annual national meeting, Mentoring in IBD XX: The Master Class, held November 15, 2019 in Toronto, Ontario.
Introduction
IBD diagnosis is not always straightforward. Main mimickers of IBD are infections, drug-induced enterocolitis, ischemia, chronic diverticular disease, immune deficiencies, intestinal neoplasia, endometriosis, systemic diseases and others. Some of the most common mimickers are discussed in this review. With respect to drug-induced enterocolitis, immune checkpoint inhibitors (ICIs: e.g., anti CTLA-4 and anti PD-1) are newer medications now in widespread use to treat a number of malignancies. The side effects of these agents are of particular concern as IBD mimickers and will be reviewed in more detail.
Differential Diagnosis of IBD
Scope of the problem
Although clinicians largely get the diagnosis of IBD correct, evidence shows a substantial subset may be initially misdiagnosed. Research using the IBSEN cohort in Norway showed that in a cohort of 739 individuals initially diagnosed with IBD, five years after the initial diagnosis, the actual diagnosis turned out not to be IBD in 44 patients (6%).(1) Among those diagnosed with ulcerative colitis (UC), the diagnosis was refuted in 32/519 patients (6.1%) and in Crohn’s disease (CD), the diagnosis was refuted in 12/221 patients (5.4%).(1) Among 40 patients who were initially diagnosed with indeterminate colitis, nine (22.5%) wound up having a non-IBD diagnosis five years later. Among the 64 patients with initially “possible IBD”, 32 (50%) had a non-IBD diagnosis five years later.
Differential diagnosis of a patient with suspected IBD
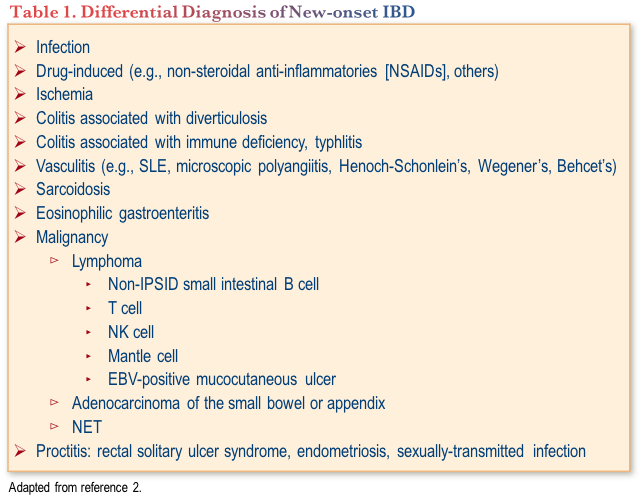
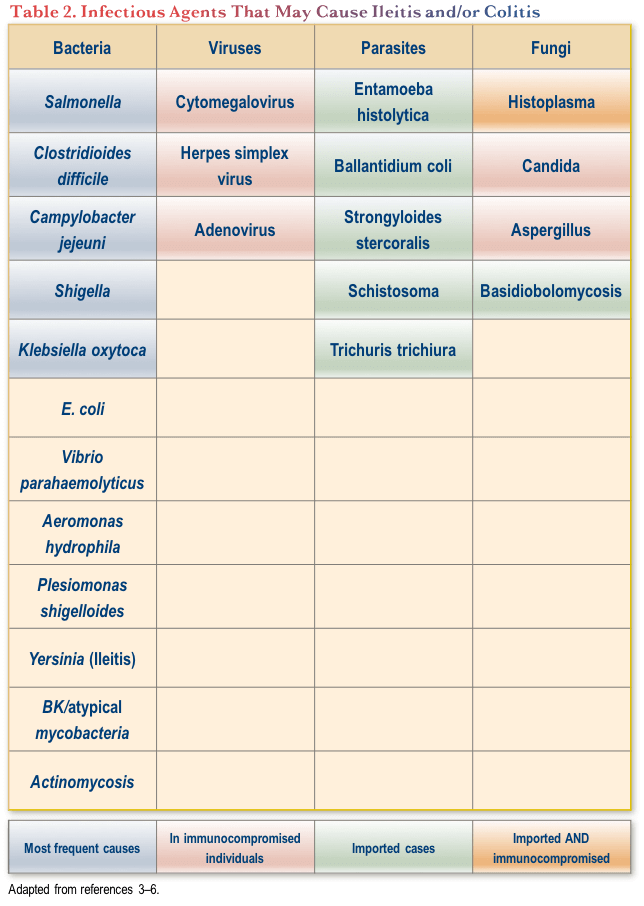
The differential diagnosis for suspected IBD is extensive (Table 1).(2) With respect to infection, the most common bacterial pathogens implicated in ileitis and/or colitis are Salmonella, C. difficile, Campylobacter jejuni, Shigella and Klebsiella oxytoca. Other potential bacterial, viral, parasitic and fungal causes are shown in Table 2.
Distinguishing an infectious cause from an inflammatory cause is, in theory, straightforward. For an infectious cause, one would see a positive stool culture and a favourable evolution with antimicrobials (e.g., fluoroquinolone ± metronidazole, azithromycin). For those with IBD, there would be a negative stool culture, no improvement with antimicrobials and colonic biopsies would show crypt distortion, basal plasmocytosis, cryptitis and/or crypt abscess.
In practice, however, there are several complicating factors. There are many bacteria that would not be detected by stool culture. Furthermore, the classic features of IBD may not be present during the earliest phases of the acute presentation.
One of the infectious causes that has been a particular focus of research is intestinal tuberculosis (TB). A meta-analysis published in 2017 provided a list of significant characteristics that help distinguish this entity from IBD.(7) With intestinal TB, one might expect the clinical presentation to include fever and/or night sweats, which are not characteristic of CD. On imaging, intestinal TB shows short segmental involvement, while endoscopy may show transverse ulcers, a patulous ileocecal (IC) valve, and cecal and/or IC valve involvement. The histology of intestinal TB includes large, confluent granulomas, multiple granulomas per section, submucosal granulomas, lymphocyte cuffing and/or ulcers lined by histiocytes. Finally, patients with intestinal TB would have a positive IGRA test.
Differential Diagnosis of IBD Relapse in a Patient with Known IBD
The differential diagnosis of relapse of symptoms in a patient with known IBD includes infection, malignancy (e.g., lymphoma, adenocarcinoma, NETs), ischemia and irritable bowel syndrome (IBS). The most common infections among patients with IBD are mostly the same as those listed above for new onset IBD: Salmonella, C. difficile, Campylobacter jejeuni, E. coli and Aeromonoas hydrophila are potential bacterial causes, while cytomegalovirus (CMV) and norovirus are the most common viral causes. Parasites may also be considered depending on the individual’s travel history.(3-6)
Differential Diagnosis of IBD: Discussion
Patients with an incorrect diagnosis may be prescribed inappropriate medication regimens, which may in turn be associated with significant and even disastrous consequences. In the current era of IBD therapy, where biologic medications are often prescribed, an incorrect diagnosis may also be financially costly for patients and/or the healthcare system. The differential diagnosis is sometimes difficult, with the main considerations being infection, ischemia and neoplasia. These other possibilities should always be kept in mind, and should receive particular consideration among migrants, individuals with vascular disease, refractory patients and those with atypical presentations.
Drug-induced IBD Mimickers
There are several pharmacotherapies that have been conclusively associated with presentations mimicking IBD. These include NSAIDs, mycophenolate, gold compounds, ICIs and other novel oncologic therapies (e.g., idelalisib, duvelisib).(8–10) ICIs currently in use in Canada include the PD-1 inhibitors nivolumab and pembrolizumab, the PD-L1 inhibitors atezolizumab and avelumab and the CTLA-4 inhibitor ipilimumab.(11) These agents, which are indicated for the treatment of several different malignancies, enhance T-cell activity, and therefore stimulate anti-cancer immunity. This mechanism of action, however, can also cause immune-related adverse effects (irAEs), including those affecting the gastrointestinal (GI) tract.(12)
The irAE profiles of the different types of ICIs are distinct from one another. The most common anti-PD-1-related irAEs, for example, are cutaneous, endocrine and pulmonary, while the most common with anti-CTLA-4 therapy are GI, cutaneous and hypophysitis.(13) Notably, the two types of agents are commonly prescribed together (nivolumab + ipilimumab). The combination is associated with an even greater risk of irAEs, including GI toxicity. The reported incidence of diarrhea with anti-PD-1 therapy alone is in the range of 11–17%, while for anti-CTLA-4 or the combination of the two, the incidence is in excess of 30%.(14–21) The incidence of ICI-related colitis is between 0.3 and 3% with anti-PD-1 therapy, 8–11% with anti-CTLA-4 and 13.6% with the combination.(14–21)
Risk factors for enterocolitis with ICIs, particularly with anti-CTLA-4, include the dose of the agent, concomitant NSAID use, pre-existing IBD, and a microbiome enriched with Firmicutes and poor in Bacteroidetes.(12) The tumour type also plays a role: GI irAEs are more common with anti-PD-1 agents among patients with melanoma compared to those with non-small-cell lung cancer or renal cell carcinoma.(12)
Anti-CTLA-4-related GI toxicities
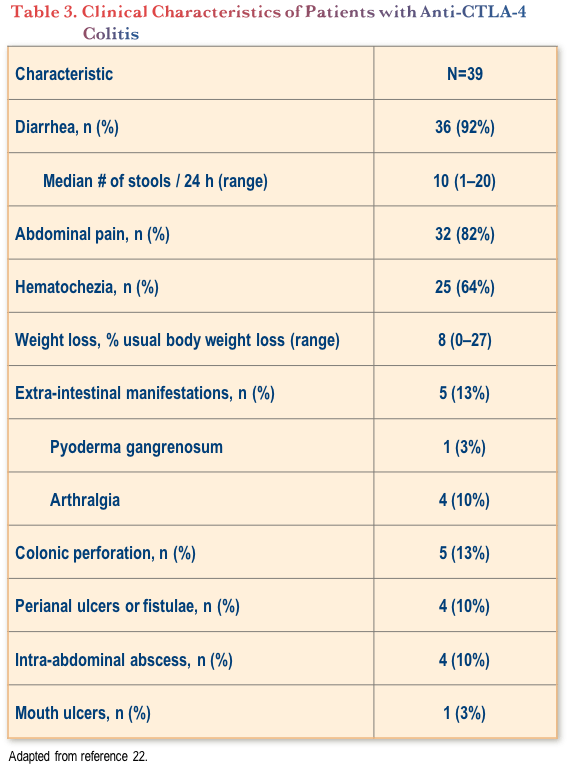
The phenotype of anti-CTLA-4-induced colitis has been well described in a study of a group of 39 patients treated with ipilimumab who experienced this irAE.(22) (Table 3) Notably, almost all the patients experienced diarrhea (36/39 patients, with a median of 10 stools per 24 hours). Hematochezia and abdominal pain were also quite common, in 25/39 (64%) and 32/39 (82%) of patients, respectively.(22)
The endoscopic observations from this study showed that approximately two-thirds of patients (23/35 with endoscopy) had extensive colitis. Almost all patients had lesions that could be reached by flexible sigmoidoscopy. Ileal involvement was observed in 5/25 patients (20%). Most patients (79%) had ulcerations noted on endoscopy, while erosions (13%) and erythema (8%) were less common.(22)
The recommended workup of a patient on ICI therapy who presents with diarrhea includes serum electrolytes and creatinine, CBC, CRP, albumin and fecal calprotectin. In addition, testing should be conducted for stool enteropathogens and C. difficile toxin. Because patients who develop severe ICI colitis may require treatment with infliximab, screening for TB, hepatitis B and HIV is also recommended.(12)
Management of anti-CTLA-4-induced colitis is similar to protocols used for acute colitis.(13) The agent should be stopped and IV corticosteroids initiated (1 to 2 mg/kg), followed by close medical and surgical supervision. The decision for subsequent therapeutic course should be made at day 3 to 7, with responders having their steroid tapered over 8–12 weeks, and non-responders and relapsers treated with infliximab.(13) Notably, for any patients who relapse or demonstrate corticosteroid resistance, the differential diagnosis should again be considered.
In the study of the 39 patients with CTLA-4-induced colitis, there was one death recorded; this was an 83-year-old man with metastatic melanoma who received high-dose intravenous steroids for 8 days and improved clinically, but he subsequently quickly deteriorated. A spontaneous colonic perforation and an abscess were found and he underwent subtotal colectomy with Hartmann’s procedure; he died postoperatively.(22)
Of the remaining 38 patients, three had spontaneous favourable evolution without intervention and 35 received medical treatment with systemic corticosteroids (mean dose 60 mg/d). Of these, 14 had a durable benefit, 14 had a partial response and 7 failed to respond. Most of those who did not respond received infliximab, while six patients underwent colectomy.(22)
In addition to colitis, ICI therapy can also be associated with severe diarrhea that may require intervention and supportive care. The severity of the ICI-induced diarrhea is stratified by the National Cancer Institute’s Common Terminology Criteria for adverse events (CTCAE).(23) Severe cases are defined as grade 3 (increase in stool number ≥7/day, incontinence, hospitalization or severe increase in stomal output compared to normal) or grade 4 (life-threatening complication; need for emergency intervention).(23)
For lower grade diarrhea (e.g., grade 1), the anti-CTLA-4 agent can be continued and supportive care added (e.g., loperamide, rehydration, budesonide or prednisone in selected cases, supervision).(13)
Anti-PD-1-related GI toxicities
GI toxicities associated with anti-PD-1 ICIs are less frequent and less severe than those associated with anti-CTLA-4.(12) Anti-PD-1-related GI toxicities have also been evaluated in a group of patients referred to a gastroenterology unit for a suspected GI irAE.(24) Among these 45 patients, half had a differential diagnosis (11 tumor-related symptoms [e.g., intestinal metastases], eight with self-limited acute diarrhea with normal workup and three with other diagnoses). Three other patients were excluded from the analysis (one refused endoscopy, one died quickly after admission and one had an association with anti-CTLA-4 therapy. The clinical picture among the 20 remaining patients with confirmed irAE was diverse: eight cases of acute colitis, seven microscopic colitis, four with gastroduodenal inflammation and one pseudo-obstruction.(24) The phenotype of acute colitis was similar to that seen among patients with anti-CTLA-4 related colitis. Forty per cent of patients with diarrhea under anti-PD-1 monotherapy had normal endoscopic findings.(24)
Can We Rechallenge with ICI after Immune-related GI toxicities?
The risk of recurrent GI irAE during a second line of ICI therapy has been reported in the range of 23–32%.(25,26) Risk factors include the use of anti-CTLA-4 in second line, the requirement for immunosuppressive therapy for the first episode and the first-line use of anti-PD-1. The decision to reintroduce ICI should be made on a case-by-case basis and discussed within a multidisciplinary team.(25,26)
Conclusions
The differential diagnosis of IBD is extensive, including infection, ischemia, chronic diverticular disease, immune deficiencies, intestinal neoplasia and, importantly, drug-induced colitis. ICIs have improved the treatment of several cancers, but are also associated with immune related colitis. This is more frequently observed and also more severe among those patients treated with ipilimumab (anti-CTLA-4) in monotherapy or in combination with an anti-PD-1 agent (e.g., nivolumab, pembrolizumab). Current management of patients with ICI-induced GI toxicity should include refutation of differential diagnoses, assessment of severity, corticosteroids and rapid introduction of infliximab in non-responders.
Clinical Case
A 36-year-old female presents to your emergency room with abdominal pain, worsening bloody diarrhea (eight to 10 bowel movements [BMs]/day), and a five-pound weight loss over the past two weeks. She denies sick contacts or recent travel. She has been on antibiotics for a urinary tract infection. She has a cousin and an uncle with histories of Crohn’s disease. Medical history is significant for a diagnosis of metastatic melanoma.
On examination:
- Temperature: 36.8°C
- BP: 104/56 mmHg
- HR: 102 bpm
Abdomen is tender to palpation with localized peritonitis. Stools (three days ago) were negative for C. difficile toxin. C&S and O&P are pending.
Investigations in ER show:
- WBC: 10.4 x109/L
- Hemoglobin: 109 g/L
- MCV: 84.2 fL
- Platelets: 438 x 109/L
- CRP: 45.2 mg/L
- Creatinine: 104 μmol/L (baseline 70)
- Abdominal X-ray: Diffuse colonic wall thickening, no free air or significant dilation
The ER doctor calls you for consultation and admission and informs you the patient is on a new chemotherapy regimen consisting of a combination of ipilimumab and nivolumab.
Commentary
At this point, both CT imaging and endoscopy would be useful to try to get a better understanding of what is going on with this patient.
You are aware that the new immune checkpoint inhibitors (ICI) that are being used to treat various malignancies can be associated with immune-related adverse events, including colitis.(27–29) Estimates of incidence of immune-mediated colitis (IMC) have ranged from 1%–25% with these agents.(27) Combination therapy with both ipilimumab (anti-CTLA4) and nivolumab (anti PD-1) is more effective than monotherapy but is associated with in increased frequency and severity of GI symptoms, including colitis, compared with either agent alone.(27)
Current recommendations for people taking checkpoint inhibitor therapy, and who experience persistent grade 2 or above diarrhea or abdominal pain, are infectious work up and colonoscopy with biopsies.(27) Ipilimumab-induced colitis most often involves lesions of the rectum and sigmoid, so flexible sigmoidoscopy is usually sufficient for diagnosis. Infectious causes of diarrhea should be ruled out with the first presentation of diarrhea or abdominal pain in patients treated with ICI therapy. Stool should be sent for standard microbiological examinations, including stool ova and parasites, bacterial culture, and C. difficile testing.(27)
Endoscopic features of IMC range from normal appearing mucosa to erosions, erythema, and loss of vascular pattern, to ulcerations. Symptom severity does not correspond with endoscopic appearance.(27,28) Gastrointestinal metastases are another, less common, possibility; these should also be ruled out as a potential etiology of symptoms.(27) Abdominal CT can also be used to rule out colonic perforation, which is a rare but well-documented (and potentially fatal) adverse event.(27)
Case Evolution
She was started on ipilimumab + nivolumab six weeks ago (she has received the first two doses). You suspect an immune-related adverse event (irAE) and decide to admit her to hospital and perform a flexible sigmoidoscopy the same day.
Endoscopy shows a Mayo 2–3 colitis with some rectal sparing. You take biopsies for histopathology and to rule out CMV and request that they be rushed. A CT of the abdomen confirms a pancolitis but no perforation, abscess or megacolon.
Commentary
Histologically, checkpoint-inhibitor colitis is commonly associated with features of acute colitis such as increased cellularity of the lamina propria with mononuclear cells, intraepithelial neutrophilic infiltrates or crypt abscesses, and an increased number of apoptotic cells in crypts.(27) While waiting for the histologic results to return, however, this patient has significant GI symptoms and should be treated empirically:(27,29)
- For mild grade 1 diarrhea (<4 stools/day above baseline): continue ICI therapy with symptomatic treatment of diarrhea with loperamide and electrolyte repletion.
- For grade 2 diarrhea or colitis (4–6 stools per day above baseline, abdominal pain, or blood or mucus in the stool), checkpoint inhibitor therapy should be withheld, and oral corticosteroids initiated at 0.5–1 mg/kg per day if symptoms persist for >1 week and tapered over 1–2 months.
- For severe grade 3 or 4 toxicity (≥7 stools above baseline per day or the presence of peritoneal signs with an ileus and fever consistent with bowel perforation), checkpoint inhibitor therapy should be permanently discontinued. Patients should be hospitalized for intravenous fluid resuscitation and expedited initial workup and treatment. Systemic corticosteroids are initiated at 1–2 mg/kg per day (prednisone or equivalent) once bowel perforation is excluded and C. difficile infection is ruled out.
Case Evolution
This patient has significant diarrhea/colitis and so you do not wait for the biopsies. As you suspect checkpoint inhibitor colitis, you start intravenous methylprednisolone 1 mg/kg/day. Over the next 72 hours, the patient does not show a significant response to therapy.
Commentary
Overall, one-third to two-thirds of patients with ICI colitis either do not respond to high-dose intravenous steroids, or have a relapse requiring an increase in the corticosteroid dosage during the course of steroid tapering.(27) If there is no improvement in symptoms within three to five days of high-dose steroids, treatment with a biologic should be initiated, with infusions at the same dose continued every two weeks until the symptoms resolve.(27) Either of the IV biologic options (infliximab or vedolizumab) would be reasonable. Usually infliximab is given at 5 mg/kg initially, but guidelines also allow for an initial 10 mg/kg dose.
Case Evolution
You prescribe infliximab 5 mg/kg. Following infliximab therapy, she has a partial improvement. After six days she is better but still has four to five BMs per day—half of which are bloody—and mild abdominal cramps. Her CRP is 18 mg/L (down from 45). The biopsies are now back from pathology and show neutrophilic infiltration in lamina propria, cryptitis, prominent distension of the crypts and no CMV inclusions
Commentary
The histology findings are consistent with an irAE secondary to the checkpoint inhibitor therapy.
Continuing with the 5 mg/kg dose every two weeks is a reasonable course here, given that the symptoms are improving.(27) However, since it is only partial response, increasing to 10 mg/kg at that time would also be a reasonable option. Switching to vedolizumab is not necessary at this time, given partial response to infliximab and the potential for further response with dose intensification.
Case Evolution
You prescribe infliximab 10 mg/kg. Within 72 hours she has a good response to therapy, with two to three non-bloody bowel movements per day, no abdominal pain and a CRP of 5 mg/L. She is discharged from hospital on a tapering regimen of prednisone. You see her in your office in two weeks. The oncologist mentioned that he wished to put her back on ipilimumab + nivolumab, as her cancer had been responding to treatment.
Commentary
For immune-related adverse events of grade 3 or lower severity, guidelines allow for consideration of resuming the checkpoint inhibitor therapy once immune-related symptoms have resolved to grade 1 or lower.(27)
Some experts advocate restarting only the anti-PD1 component of the immune checkpoint therapy (nivolumab in this case) for those who experience significant immune-related toxicity on the combination of anti-CTLA4 (i.e., ipilimumab) and anti-PD1.(27)
Maintenance infliximab is not indicated as prophylaxis against checkpoint-inhibitor colopathy. Furthermore, prophylactic systemic steroids have been evaluated for the prevention of irAEs with checkpoint inhibitors, without any significant impact observed.(27)
References
-
Henriksen M, Jahnsen J, Lygren I, et al. Change of diagnosis during the first five years after onset of inflammatory bowel disease: results of a prospective follow-up study (the IBSEN study). Scand J Gastroenterol. 2006;41:1037–43.
-
Dilauro S, Crum-Cianflone NF. Ileitis: When It Is Not Crohn’s Disease. Curr Gastroenterol Rep. 2010;12(4):249–58.
-
Axelrad JE, Joelson A, Green PH, et al. Enteric Infections Are Common in Patients With Flares of Inflammatory Bowel Disease. Am J Gastroenterol. 2018;113(10):1530–9.
-
Sager K, Alam S, Bond A, et al. Review article: cytomegalovirus and inflammatory bowel disease. Aliment Pharmacol Ther. 2015;41(8):725–33.
-
Lin WC, Chang CW, Chen MJ, et al. Challenges in the Diagnosis of Ulcerative Colitis With Concomitant Bacterial Infections and Chronic Infectious Colitis. PLoS One. 2017;12(12):e0189377.
-
Lobatón T, et al. Bacterial Intestinal Superinfections in Inflammatory Bowel Diseases Beyond Clostridum difficile. Inflamm Bowel Dis. 2016;22(7):1755–62.
-
Limsrivilai J, Shreiner AB, Pongpaibul A, et al. Meta-Analytic Bayesian Model For Differentiating Intestinal Tuberculosis From Crohn’s Disease. Am J Gastroenterol. 2017;112(3):415–27.
-
Liu TC, Amorosino MS, Cerda S. Mycophenolate Mofetil-Associated Enterocolitis. Gastrointest Endosc. 2006;63(4):707–8.
-
Weidner AS, Panarelli NC, Geyer JT, et al. Idelalisib-associated Colitis: Histologic Findings in 14 Patients. Am J Surg Pathol. 2015;39(12):1661–7.
-
Flinn IW, O’Brien S, Kahl B, et al. Duvelisib, a Novel Oral Dual Inhibitor of PI3K-δ,γ, Is Clinically Active in Advanced Hematologic Malignancies. 2018;131(8):877–87.
-
Health Canada. Drug Products Database. Online at: https://www.canada.ca/en/health-canada/services/drugs-health-products/drug-products/drug-product-database.html. Accessed May 2020.
-
Soularue E, Lepage P, Colombel J-F, et al. Enterocolitis Due to Immune Checkpoint Inhibitors: A Systematic Review. Gut. 2018;67(11):2056–67.
-
Haanen JB, Carbonnel F, Robert C, et al. Management of toxicities from immunotherapy: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2017;28(suppl_4):iv119–iv142.
-
Baxi S, Yang A, Gennarelli RL, et al. Immune-related Adverse Events for anti-PD-1 and anti-PD-L1 Drugs: Systematic Review and Meta-Analysis. 2018;360:k793.
-
De Velasco G, Je Y, Bossé D, Awad MM, et al. Comprehensive Meta-analysis of Key Immune-Related Adverse Events from CTLA-4 and PD-1/PD-L1 Inhibitors in Cancer Patients. Cancer Immunol Res. 2017;5(4):312–8.
-
Khoja L, Day D, Wei-Wu Chen T, et al. Tumour- and class-specific patterns of immune-related adverse events of immune checkpoint inhibitors: a systematic review. Ann Oncol. 2017;28(10):2377–85.
-
Komaki Y, Komaki F, Yamada A, et al. Meta-Analysis of the Risk of Immune-Related Adverse Events With Anticytotoxic T-Lymphocyte-Associated Antigen 4 and Antiprogrammed Death 1 Therapies. Clin Pharmacol Ther. 2018;103(2):318–31.
-
Tandon P, Bourassa-Blanchette S, Bishay K, et al. The Risk of Diarrhea and Colitis in Patients With Advanced Melanoma Undergoing Immune Checkpoint Inhibitor Therapy: A Systematic Review and Meta-Analysis. J Immunother. 2018;41(3):101–8.
-
Wang DY, Ye F, Zhao S, et al. Incidence of immune checkpoint inhibitor-related colitis in solid tumor patients: A systematic review and meta-analysis. Oncoimmunology. 2017;6(10):e1344805.
-
Wang PF, Chen Y, Song SY, et al. Immune-Related Adverse Events Associated with Anti-PD-1/PD-L1 Treatment for Malignancies: A Meta-Analysis. Front Pharmacol. 2017;8:730.
-
Zhang B, Wu Q, Zhou YL, et al. Immune-related adverse events from combination immunotherapy in cancer patients: A comprehensive meta-analysis of randomized controlled trials. Int Immunopharmacol. 2018;63:292–8.
-
Marthey L, Mateus C, Mussini C, et al. Cancer Immunotherapy with Anti-CTLA-4 Monoclonal Antibodies Induces an Inflammatory Bowel Disease. J Crohns Colitis. 2016;10(4):395–401.
-
S. Department of Health and Human Services. Common Terminology Criteria for Adverse Events (CTCAE) Version 5.0. Online at: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/CTCAE_v5_Quick_Reference_5x7.pdf. Accessed May, 2020.
-
Collins M, Michot JM, Danlos FX, et al. Inflammatory Gastrointestinal Diseases Associated With PD-1 Blockade Antibodies. Ann Oncol. 2017;28(11):2860–5.
-
de Malet A, Antoni G, Collins M, et al. Evolution and Recurrence of Gastrointestinal Immune-Related Adverse Events Induced by Immune Checkpoint Inhibitors. Eur J Cancer. 2019;106:106–14.
-
Abu-Sbeih H, Ali FS, Naqash AR, et al. Resumption of Immune Checkpoint Inhibitor Therapy After Immune-Mediated Colitis. J Clin Oncol. 2019;37(30):2738–45.
-
Som A, Mandaliya R, Alsaadi D, et al. Immune checkpoint inhibitor-induced colitis: A comprehensive review. World J Clin Cases. 2019;7(4):405–18.
-
Trac B, Chen HH, Muhlbauer A, et al. IpiColitis: ipilimumab-induced colitis with a wide spectrum of histological features. Am J Digest Dis. 2018;5(1):1–11.
-
Weber JS, Postow M, Lao CD, et al. Management of Adverse Events Following Treatment With Anti-Programmed Death-1 Agents. Oncologist. 2016;21(10):1230–40.
Editor-in-Chief
John K. Marshall, MD MSc FRCPC AGAF, Director, Division of Gastroenterology, Professor, Department of Medicine, McMaster University, Hamilton, ON
Contributing Editor
Franck Carbonnel, MD, Professor of Gastroenterology, University Paris Sud, Head, Gastroenterology Department, University Hospital of Kremlin Bicȇtre, Paris, France
Mentoring in IBD Curriculum Steering Committee
Alain Bitton, MD FRCPC, McGill University, Montreal, QC
Anne M. Griffiths, MC FRCPC, University of Toronto, Toronto, ON
Karen I. Kroeker, MD MSc FRCPC, University of Alberta, Edmonton, AB
Cynthia Seow, MBBS (Hons) MSc FRACP, University of Calgary, Calgary, AB
Jennifer Stretton, ACNP MN BScN, St. Joseph’s Healthcare, Hamilton, ON
IBD Dialogue 2020·Volume 16 is made possible by unrestricted educational grants from…
![]()


![]()
Published by Catrile & Associates Ltd., 1B-391 Berkeley Street, Toronto, ON M5A 2X8
(c) Catrile & Associates Ltd., 2020. All rights reserved. None of the contents may be reproduced in any form without prior written permission from the publisher. The opinions expressed in this paper are those of the authors and do not necessarily reflect the opinions or recommendations of the sponsors, the grantor, or the publisher.