
Update on Vaccine Preventable Illness in IBD
Update on Vaccine Preventable Illness in IBD
January 25, 2022
Issue 01
Mentoring in IBD is an innovative and successful educational program for Canadian gastroenterologists that includes an annual national meeting, regional satellites in both official languages, www.mentoringinibd.com, an educational newsletter series, and regular electronic communications answering key clinical questions with new research. This issue is based on the presentation made by Dr. Jennifer Jones, at the 22nd annual national meeting, Mentoring in IBD XXII: The Master Class, held virtually, November 5, 2021.
Optimal Imaging Technologies for Small Bowel CD: The Radiologist’s Perspective (Dr. Luís Guimarães)
Roles of Enterography in Small Bowel CD
Clinical experience has shown that there can be a major disconnect between the clinical impression of a patient with Crohn’s disease (CD), what is seen on endoscopy and what can be seen by advanced imaging (e.g., magnetic resonance enterography [MRE] or computed tomography enterography [CTE]). An asymptomatic patient may, for example, display signs of advanced disease (e.g., strictures, penetrating disease, fistula) on imaging. Similarly, a patient with a normal looking bowel on endoscopy might show other signs of more advanced disease (e.g., mural thickening, mild stricturing) on MRE.
With these disconnects in mind, the following review discusses optimal use of current imaging and endoscopic techniques, from the perspectives of a radiologist and a gastroenterologist.
The most recent evidence-based expert consensus recommendations for the use of imaging in CD was published in 2018.(1) The Consensus Recommendations for Evaluation, Interpretation, and Utilization of Computed Tomography and Magnetic Resonance Enterography in Patients With Small Bowel Crohn’s Disease were endorsed by the American Gastroenterological Association, the Society of Abdominal Radiology (U.S.) and the Society for Pediatric Radiology (U.S.).(1)
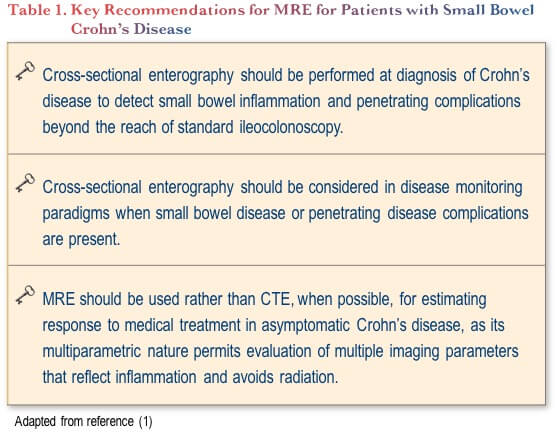
Three key recommendations from this paper spell out the role of cross-sectional enterography (CT and MR enterography) for small bowel disease (Table 1). Cross-sectional enterography should always be performed for staging at diagnosis to detect inflammation and penetrating complications beyond the reach of standard ileocolonoscopy. Cross-sectional enterography should also be considered for monitoring, and MRE is preferred over CT enterography to assess response to medical treatment.
Imaging the entire bowel is, therefore, critical to understand the total inflammatory burden of any given patient. One rationale for the use of advanced imaging at diagnosis (in addition to endoscopy) is the phenomenon of endoscopic skipping, first described in 2012.(2) While small bowel CD often involves the terminal ileum (TI), skipping of the distal TI can occur, which would lead to negative results from ileocolonoscopy. This was shown in an investigation of 153 patients with small bowel CD who had undergone both ileoscopy and CTE. Of the 153, 67 (44%) were reported to have a normal appearance on ileoscopy. However, when they were examined by CTE, 36 (54%) of those individuals with normal endoscopic appearance had active, small-bowel CD. Among those individuals, the disease had “skipped” the distal ileum in 11 patients (30.6%), 23 patients had disease in the TI—which had been assessed by endoscopy—but only intramural (not mucosal) disease (therefore not seen with endoscopy), and two patients had only proximal CD, out of the reach of the scope.(2)
Imaging is also essential for identifying stricturing and penetrating disease, which can be missed by endoscopy. Up to one-third of patients with CD have evidence of stricturing or penetrating complications at diagnosis, but these are underdiagnosed without the use of cross-sectional imaging.(3) In a prospective study of 273 patients with established or suspected CD who underwent CTE, their physicians were asked to develop a treatment plan prior to getting the results of the imaging.(4) After receiving the CTE results, providers were asked if the results altered their management plans. More than half (139/273; 51%) did change management, including exclusion of CD in 36% of those with suspected CD at baseline. Similar results had previously been seen in a smaller, retrospective study.(5)
With respect to monitoring, imaging is an important tool to assess response to treatment. Changes in mucosal hyper-enhancement and mural thickening, in particular, are easy to visualize using CTE or MRE. Mucosal healing, one of the key goals of therapy in IBD,(6) can also be assessed with imaging.(7,8) One study of 48 patients with active CD and ulcers in at least one ileocolonic segment included both ileocolonoscopy and MRE at baseline and 12 weeks after completing treatment. The investigator reported a strong correlation (r=0.81, P<0.001) between the Crohn’s Disease Endoscopic Index of Severity (CDEIS) and the Magnetic Resonance Index of Activity (MaRIA).(8)
Cross-sectional enterography is even more essential in monitoring to evaluate transmural response to treatment (rather than only mucosal healing). Transmural healing has been associated with better long-term outcomes than mucosal healing in small bowel CD.(9,10) The utility of adding this assessment to monitoring response was evaluated among 214 patients with CD with a magnetic resonance enterography (MRE) and colonoscopy performed within a 6-month interval. Compared to those who only demonstrated mucosal healing by colonoscopy, but not transmural healing by MRE, those who demonstrated both mucosal healing and transmural healing were significantly less likely to require an escalation of medical treatment (15.2% vs. 36.5%, P=0.027) or surgery (0% vs. 11.5%, P=0.047).(10)
New Technologies: The Gastroenterologist’s Perspective (Dr. Bincy Abraham)
Clinical Case
A 19-year-old male presents with generalized worsening abdominal pain for 2 months, which caused him to delay starting his university studies. He eventually started classes, but moved his schedule to night classes only to accommodate his disease, as his pain is worse in the mornings. He has daily formed bowel movements without hematochezia, mucus or melena. His weight is stable, and he has a normal appetite. He is not a strict vegetarian, but states that he avoids eating meat most days. He has not experienced any nausea, vomiting, heartburn or regurgitation. He does not drink alcohol, has never smoked and does not use any other recreational drugs.
He has been prescribed sucralfate, esomeprazole and dicyclomine, all of which have been ineffective for his abdominal pain. He was recently prescribed amitriptyline, but due to prior episodes of depression and reports of suicidal ideation on other antidepressants, he declined to start taking amitriptyline. His current medications are now only cetirizine 10 mg as needed for seasonal allergies, and ibuprofen 600 mg as needed for pain.
There is no GI disease history in the family. The only notable family history is that his sister also suffers from depression.
Review of systems shows that he has arthralgias of the knee and hip. He has previously been evaluated by an orthopaedic surgeon who referred him for physical therapy, and by a rheumatologist who diagnosed him with non-specific arthritis and recommended the use of NSAIDs as needed.
Except for a flat affect, his physical examination was unremarkable, with normal vital signs and normal BMI. Of note, abdominal exam revealed a soft, nontender abdomen, with normal bowel sounds, no distension and no mass. The examination of the joints was also unremarkable.
Previous testing about a year prior due to similar symptoms included a negative celiac panel (tissue transglutaminase antibodies [TTG-IgA] <1), and a negative urea breath test for H. pylori. Esophagogastroduodenoscopy showed mild erythema of the distal esophagus with biopsies consistent with acid reflux. The proximal esophagus, stomach and duodenum were all endoscopically and histologically normal, including gastric biopsy negative for H. pylori. Colonoscopy showed normal mucosa of the entire colon and terminal ileum. However, mucosal biopsies from the cecum showed mild focal acute colitis, rectosigmoid biopsy showed normal mucosa with a single granuloma in the lamina propria, and all other biopsies (ileum, ascending, transverse and descending colon) were normal.
Due to these negative or nonspecific findings, an MRE was ordered but the patient could not tolerate the full amount of oral contrast for the study. The MRE did reveal mild active colitis involving a long continuous segment of rectosigmoid colon. The small bowel was normal and the scan was otherwise unremarkable. An ileocolonoscopy was thus scheduled which showed normal cecum, some erythema and small erosions in the terminal ileum and at the ileocecal valve. The entire colon however, was normal including the rectosigmoid areas. No ulcerations were noted. Biopsy of the terminal ileum showed acute ileitis. Random colon biopsies, including the rectosigmoid areas, were normal.
The diagnosis was considered to be nonspecific, with the differential including IBD and possible NSAID-induced erosions. The gastroenterologist opted to hold any NSAID use for eight weeks and further evaluate the small bowel with capsule endoscopy (CE). This showed numerous ulcerations and patchy erythema throughout the small intestine, most marked in the distal ileum and largely sparing the terminal ileum. An official diagnosis of CD was made.
Capsule Endoscopy
Among the many endoscopic and cross-sectional intestinal imaging techniques, CE proved to be the most useful in the above scenario—where other findings were nonspecific or inconclusive when disease of the upper small bowel was suspected. The technology is non-invasive and it allows for excellent magnified imaging of the small bowel, to the level of individual villi. Images are taken two per second as the capsule moves passively through the GI tract.
Limitations of this technology include the lack of ability to biopsy or take samples, and time required for the procedure. There is also the risk of capsule retention, which may require surgery. Also, if a patient has poor bowel preparation, visibility may be markedly reduced.
The general recommendation would be to use CE for diagnosis when there is a clinical suspicion of CD, but upper and lower endoscopies are negative, with or without a negative CTE/MRE.
For confirmed CD, CE can also be useful. It is significantly more sensitive than radiologic imaging for the detection of inflammatory lesions and can measure small bowel healing without radiation. Mucosal evaluation of the whole small bowel is important to identify proximal lesions associated with worse prognosis (e.g., surgery and higher risk of relapse).
Notably, there is also newer capsule technology. A PillCamTM specific for CD, has two cameras and provides direct visualization of the entire luminal tract, including the colon, in one procedure. A notable drawback of this device is the need for full bowel preparation as it is needed to visualize the entire colon.
In terms of correlation with imaging, the Lewis score used with CE has been shown to correlate modestly with both the MaRIA and Clermont scores for MRE.(11) Another study among 47 patients with established (n=32) or suspected (n=15) CD showed that the diagnostic yield with capsule endoscopy was greater (53.1% had their pre-test Montreal classification changed) than with MRE (12.7% changed).(12) The difference was largely due to the superiority of CE in detecting small bowel lesions (mainly superficial and proximal).
More comparative information comes from a 2017 meta-analysis including 13 prospective studies that compared the diagnostic yields of capsule endoscopy, MRE or small bowel intestinal contrast ultrasound (SICUS) for evaluation and monitoring of CD.(13) In this analysis, CE was found to have a diagnostic yield comparable to both other modalities. However, for small-bowel CD in particular, CE was found to be superior to MRE, with an odds ratio of 2.79 (95% CI 1.2 to 6.48).
Patient comfort is another important consideration. CE is more acceptable to patients, with less discomfort than MRE, during preparation and during the procedure itself.(14) Patients are also more likely to agree to have repeat CE than repeat MRE.(14)
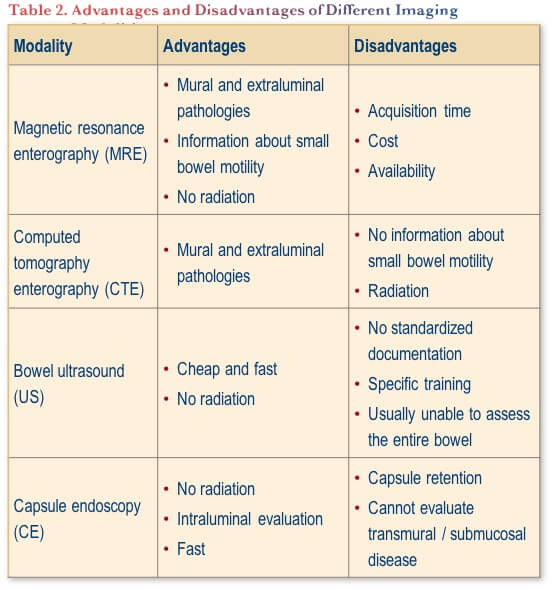
Table 2 summarizes the advantages and disadvantages of different imaging modalities for small bowel CD. Note that exposure to ionizing radiation is a concern, given that CD is a lifelong chronic disease and individuals can be scanned a number of times over the course of their disease and accrue very high radiation exposure.(15)
CTE vs. MRE: What Do We Need to Know? (Dr. Luís Guimarães)
As mentioned above, one of the recommendations from the recent Consensus Recommendations for Evaluation, Interpretation, and Utilization of Computed Tomography and Magnetic Resonance Enterography in Patients With Small Bowel Crohn’s Disease was that “MRE should be used rather than CTE, when possible, for estimating response to medical treatment in asymptomatic Crohn’s disease, as its multiparametric nature permits evaluation of multiple imaging parameters that reflect inflammation and avoids radiation.” (1)
That said, the level of evidence for this recommendation is reported as low. More importantly, the reality of our situation in Canada is that timely access to MRE can be difficult, while CT, a robust, reliable and sensitive imaging tool, is typically more available to clinicians and their patients. The image quality is also more consistently readable than is the case with MRE, where peristalsis often results in blurred images that cannot be interpreted.
With respect to radiation, this was a much bigger concern with older CT techniques, where the average exposure was in the range of 10–25 mSv per test.(15,16) Modern CT scans can be performed with less than 2 mSv of radiation and no loss of sensitivity, through use of an iterative reconstruction technique.(17,18)
Given the low radiation exposure associated with newer CT techniques, there is the potential for this modality to be used more frequently for the assessment of response to treatment and to monitor disease activity, and also to assess strictures, particularly if MRE is not readily available.
While MRE has been shown to be accurate for detecting the presence of severe fibrosis in CD lesions,(19) preliminary work shows that this may potentially also be accomplished with CTE if MRE is not accessible, but this is not well established at the moment. A study is currently underway using a CTE technique that involves a second acquisition covering only the stricture at seven minutes. The patients then undergo an MRE. There has been good correlation between the two modalities.
Conclusions
Both CTE and MRE have established and evolving roles in CD. The evolution of transmural healing as a treatment target will lead to an increased role for enterography. The revolution in radiation dose with CTE repositions this modality in CD, particularly where access to MRE is limited.
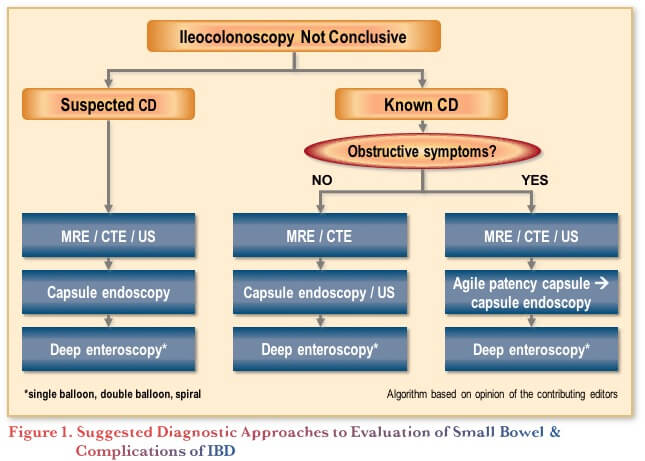
Figure 1 shows a possible algorithmic approach to the evaluation of the small bowel among patients with an inconclusive ileocolonoscopy. In all cases, local expertise and availability should be considered. For all patients, one might first consider cross-sectional imaging with MRE or CTE, followed by consideration of CE, and then deep enteroscopy (e.g., balloon, spiral) if necessary. Ultrasound may also be useful where the expertise is available. Note that among those with known CD and obstructive symptoms, an agile patency capsule should first be used to determine whether the CE will pass through.
References
-
Bruining DH, Zimmermann EM, Loftus EV Jr, et al. Consensus Recommendations for Evaluation, Interpretation, and Utilization of Computed Tomography and Magnetic Resonance Enterography in Patients With Small Bowel Crohn’s Disease. Gastroenterology. 2018;154(4):1172–94.
-
Samuel S, Bruining DH, Loftus EV Jr, et al. Endoscopic skipping of the distal terminal ileum in Crohn’s disease can lead to negative results from ileocolonoscopy. Clin Gastroenterol Hepatol. 2012;10(11):1253–9.
-
Peyrin-Biroulet L, Loftus EV Jr, Colombel JF, et al. The natural history of adult Crohn’s disease in population-based cohorts. Am J Gastroenterol. 2010;105(2):289–97.
-
Bruining DH, Siddiki HA, Fletcher JG, et al. Benefit of computed tomography enterography in Crohn’s disease: effects on patient management and physician level of confidence. Inflamm Bowel Dis. 2012;18(2):219–25.
-
Booya F, Akram S, Fletcher JG, et al. CT enterography and fistulizing Crohn’s disease: clinical benefit and radiographic findings. Abdom Imaging. 2009;34(4):467–75.
-
Peyrin-Biroulet L, Sandborn W, Sands BE, et al. Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE): Determining Therapeutic Goals for Treat-to-Target. Am J Gastroenterol. 2015;110(9):1324–38.
-
Hashimoto S, Shimizu K, Shibata H, et al. Utility of computed tomographic enteroclysis/enterography for the assessment of mucosal healing in Crohn’s disease. Gastroenterol Res Pract. 2013;2013:984916.
-
Ordás I, Rimola J, Rodríguez S, et al. Accuracy of magnetic resonance enterography in assessing response to therapy and mucosal healing in patients with Crohn’s disease. Gastroenterology. 2014;146(2):374–82.
-
Deepak P, Fletcher JG, Fidler JL, et al. Radiological Response Is Associated With Better Long-Term Outcomes and Is a Potential Treatment Target in Patients With Small Bowel Crohn’s Disease. Am J Gastroenterol. 2016;111(7):997–1006.
-
Fernandes SR, Rodrigues RV, Bernardo S, et al. Transmural Healing Is Associated with Improved Long-term Outcomes of Patients with Crohn’s Disease. Inflamm Bowel Dis. 2017;23(8):1403–9.
-
Kopylov U, Klang E, Yablecovitch D, et al. Magnetic resonance enterography versus capsule endoscopy activity indices for quantification of small bowel inflammation in Crohn’s disease. Therap Adv Gastroenterol. 2016;9(5):655–63.
-
González-Suárez B, Rodriguez S2, Ricart E, et al. Comparison of Capsule Endoscopy and Magnetic Resonance Enterography for the Assessment of Small Bowel Lesions in Crohn’s Disease. Inflamm Bowel Dis. 2018;24(4):775–80.
-
Kopylov U, Yung DE, Engel T, et al. Diagnostic yield of capsule endoscopy versus magnetic resonance enterography and small bowel contrast ultrasound in the evaluation of small bowel Crohn’s disease: Systematic review and meta-analysis. Dig Liver Dis. 2017;49(8):854–63.
-
Lahat A, Kopylov U, Amitai MM, et al. Magnetic resonance enterography or video capsule endoscopy – what do Crohn’s disease patients prefer? Patient Prefer Adherence. 2016;10:1043–50.
-
Desmond AN, O’Regan K, Curran C, et al. Crohn’s disease: factors associated with exposure to high levels of diagnostic radiation. Gut. 2008;57(11):1524–9.
-
Peloquin JM1, Pardi DS, Sandborn WJ, et al. Diagnostic ionizing radiation exposure in a population-based cohort of patients with inflammatory bowel disease. Am J Gastroenterol. 2008;103(8):2015–22.
-
Murphy KP, Crush L, Twomey M, et al. Model-Based Iterative Reconstruction in CT Enterography. AJR Am J Roentgenol. 2015;205(6):1173–81.
-
Rosenfeld G, Brown J, Vos PM, et al. Prospective Comparison of Standard- Versus Low-Radiation-Dose CT Enterography for the Quantitative Assessment of Crohn Disease. AJR Am J Roentgenol. 2018;210(2):W54–W62.
-
Rimola J, Planell N, Rodríguez S, et al. Characterization of inflammation and fibrosis in Crohn’s disease lesions by magnetic resonance imaging. Am J Gastroenterol. 2015;110(3):432–40.
Editor-in-Chief
John K. Marshall, MD MSc FRCPC AGAF, Director, Division of Gastroenterology, Professor, Department of Medicine, McMaster University, Hamilton, ON
Contributing Editors
Bincy P. Abraham, MD MS AGAF FACG, Associate Professor of Clinical Medicine, Weill Cornell Medical College; Adjunct Associate Professor of Internal Medicine, Texas A&M University, College of Medicine; Director, Gastroenterology Fellowship Program, Houston Methodist; Distinguished Professor and Director, Underwood Center—Fondren Inflammatory Bowel Disease Program, Houston Methodist Gastroenterology Associates, Houston, TX
Luís S. Guimarães, MD PhD, Assistant Professor, University of Toronto, Mount Sinai Hospital and University Health Network, Joint Department of Medical Imaging, Toronto, ON
Mentoring in IBD Curriculum Steering Committee
Alain Bitton, MD FRCPC, McGill University, Montreal, QC
Anne M. Griffiths, MC FRCPC, University of Toronto, Toronto, ON
Karen I. Kroeker, MD MSc FRCPC, University of Alberta, Edmonton, AB
Cynthia Seow, MBBS (Hons) MSc FRACP, University of Calgary, Calgary, AB
Jennifer Stretton, ACNP MN BScN, St. Joseph’s Healthcare, Hamilton, ON
IBD Dialogue 2020·Volume 16 is made possible by unrestricted educational grants from…
![]()


![]()
Published by Catrile & Associates Ltd.
1B-391 Berkeley Street, Toronto, ON M5A 2X8
(c) Catrile & Associates Ltd., 2020. All rights reserved. None of the contents may be reproduced in any form without prior written permission from the publisher. The opinions expressed in this paper are those of the authors and do not necessarily reflect the opinions or recommendations of the sponsors, the grantor, or the publisher.