
Obesity in IBD: Friend or Foe?
Obesity in IBD: Friend or Foe?
February 27, 2023
Issue 02
Mentoring in IBD is an innovative and successful educational program for Canadian gastroenterologists that includes an annual national meeting, regional satellites in both official languages, www.mentoringinibd.com, an educational newsletter series, and regular electronic communications answering key clinical questions with new research. This issue is based on the presentation made by Dr. Siddharth Singh, at the 23rd annual national meeting, Mentoring in IBD XXIII: The Master Class, held in Toronto on November 4, 2022.
Epidemiology and Pathophysiology of Obesity in IBD
The objectives of Dr. Singh’s presentation were to discuss the epidemiology and pathophysiology of obesity in IBD as well as the impact of obesity on the natural history, treatment response, and outcomes in patients with IBD.
This is a tale of two epidemics with increasing incidence rates of both overweight/obesity and IBD globally.1,2 While IBD was traditionally associated with weight loss, recent data suggest that 20–40% of adult patients with IBD are obese, with similar patterns seen in pediatric populations.3,4
As to whether obesity contributes to the development of IBD, a systematic review of 10 studies including 15.6 million individuals, and 23,371 cases of IBD, showed a non-linear association between being either underweight or obese and the risk of developing Crohn’s disease (CD). Specifically, there was a 25% higher risk of developing CD in obese vs. non-obese adults, while there was no association in the risk of developing ulcerative colitis (UC).5
In terms of how obesity may contribute to the pathogenesis of IBD, there are likely multiple factors involved, including dysbiosis, pro-inflammatory adipocytokines, and intestinal barrier disruption.6 In studies in animal models of atopic dermatitis, obesity has been shown to convert a classically TH2-driven inflammatory disease to a more severe TH17-driven disease that is worsened upon anti-TH2 antibody treatment, which may also be relevant for IBD.7
Impact of Obesity on Natural History of IBD
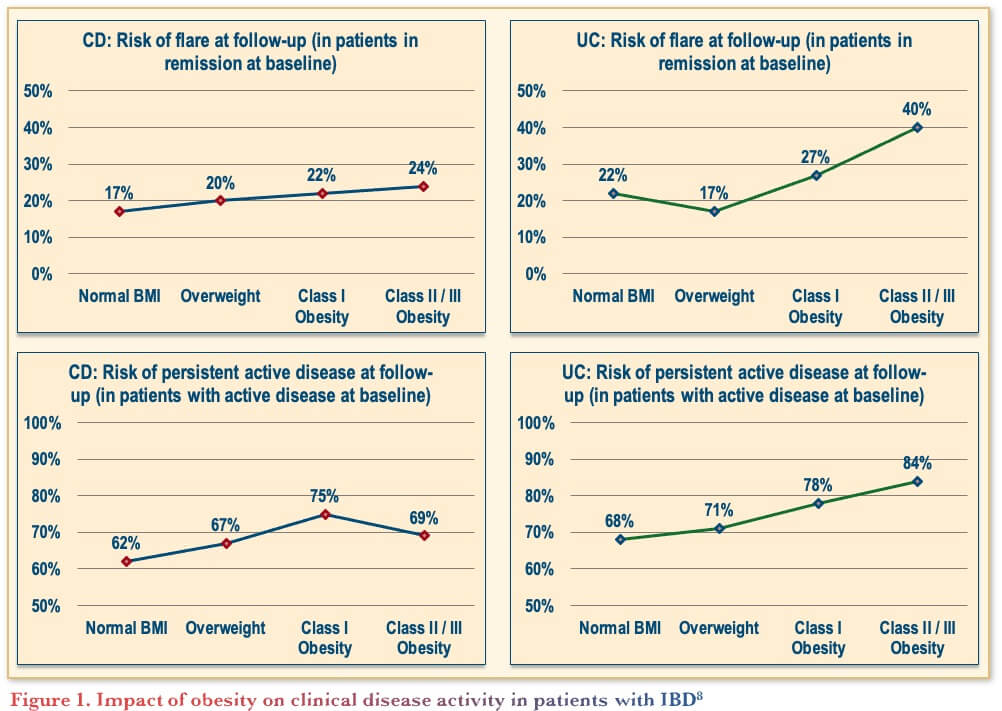
A cross-sectional and longitudinal analysis from the IBD Partners cohort included 7,296 adults with IBD (65% with CD, 20% obese). The results showed that as patients moved from normal to higher body weight there was an increased risk of persistent disease activity or disease relapse in both UC and CD (Figure 1).8
In addition, a population-based study on the prevalence and impact of obesity on disease outcomes in UC specifically showed that the prevalence of obesity increased 2–3-fold over the 40-year study period. Furthermore, each unit increase in body mass index (BMI) was associated with an increase in the risk of future corticosteroid use and hospitalization, but not surgery.9
Although most of the data focus on overall obesity, it is generally agreed that BMI is not the best way of measuring overall adiposity, so studies have also investigated the specific impact of visceral adiposity in CD. Results have demonstrated that increased visceral adiposity was associated with a more complicated high-risk phenotype and adverse outcomes in CD, for both adult and pediatric patients.10,11
Impact of Obesity on Treatment Response in IBD
Studies suggest that obesity impacts treatment response in IBD, in part because of its effect on the pharmacokinetics (exposure and absorption) of biologic agents, regardless of whether the biologic is administered by intravenous or subcutaneous routes.12,13 Thus, it is important to recognize that while weight-based dosing may be helpful, it may not fully negate the potential negative impact of obesity in patients with IBD.
In terms of the impact of obesity on treatment response in IBD, less than 10% of clinical trials of anti-TNF agents have reported outcomes stratified by BMI, and even these often assessed only dichotomous weight categories.6 Thus, a larger study was undertaken to include all immune-mediated diseases including 54 cohorts (19,372 patients; 23% obese). The results showed that obese patients have 60% higher odds of failing anti-TNF therapy OR, 1.60 (95% CI, 1.39–1.83) with a clear dose-response relationship.15
Studies in IBD include a single-center, retrospective cohort study of 160 patients with UC, including 55% on weight-based therapy (infliximab; IFX) and 45% on fixed-dose therapy (adalimumab, golimumab, vedolizumab). The results showed that a 1 kg/m2 increase in BMI was associated with a 4% higher risk of treatment failure when adjusting for age, sex, disease duration, hospitalization, prior anti-TNF therapy, steroid use, and albumin. Furthermore, a 1 kg/m2 increase in BMI was also associated with a 6% lower risk of achieving endoscopic remission, and this was consistent across therapies.14
However, looking more specifically at IFX for IBD, a pooled analysis from clinical trials found that with each 1kg/m2 increase in BMI there was no association with odds of achieving clinical remission.16 To look at additional outcome measures, a multi-center EHR-based cohort study was completed including biologic-treated patients with IBD (n=3,038; 76% treated with IFX, 12% each on vedolizumab and ustekinumab). Results showed that within 1 year of biologic initiation, hospitalization rates and IBD-related surgery were not associated with obesity, although the burden of healthcare utilization in obese patients with IBD was higher (e.g., longer hospital stay).17
Would Treating Obesity Modify Outcomes in Patients with IBD?
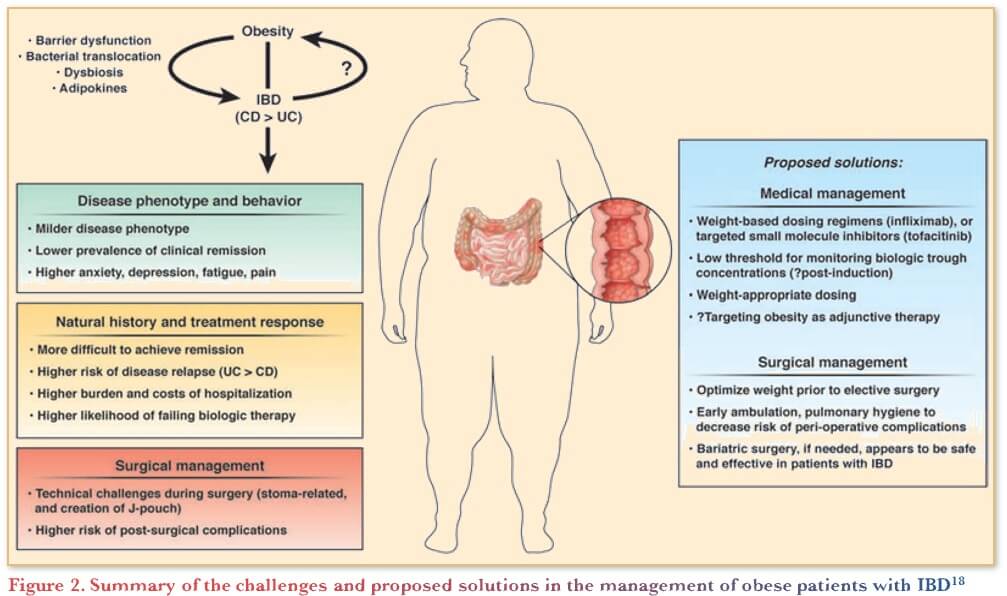
A recent review article summarizes the challenges and proposed solutions in the management of obese patients with IBD (Figure 2).18
While there are no interventional studies of intentional weight loss in IBD, trials of diet and/or lifestyle-induced weight loss in other autoimmune diseases suggest improvement in clinical outcomes with intentional weight loss.18 Specifically, studies on the use of anti-TNFs in psoriatic arthritis found that, regardless of the type of weight loss intervention, the magnitude of weight loss was associated with better outcomes in terms of minimal disease activity in overweight/obese patients.19 In addition, studies showed that bariatric surgery improved outcomes in rheumatoid arthritis (RA), with a single-center study (n=53) showing an improvement in disease activity, inflammatory markers, and RA-related medication use.20
While bariatric surgery is done infrequently in IBD, a systematic review and meta-analysis of 10 studies was undertaken including 168 patients with IBD (58% CD; 52% not on any specific IBD-related therapy; 28% on biologics). In terms of safety, 16% experienced early surgery-related adverse events, and there was a higher rate with Roux-en-Y gastric bypass (REYGB) vs. sleeve gastrectomy. In terms of efficacy, following surgery, 46% decreased their IBD medications, and 10% experienced therapeutic escalation, although further study is needed to determine the safest bariatric surgery method in IBD.21
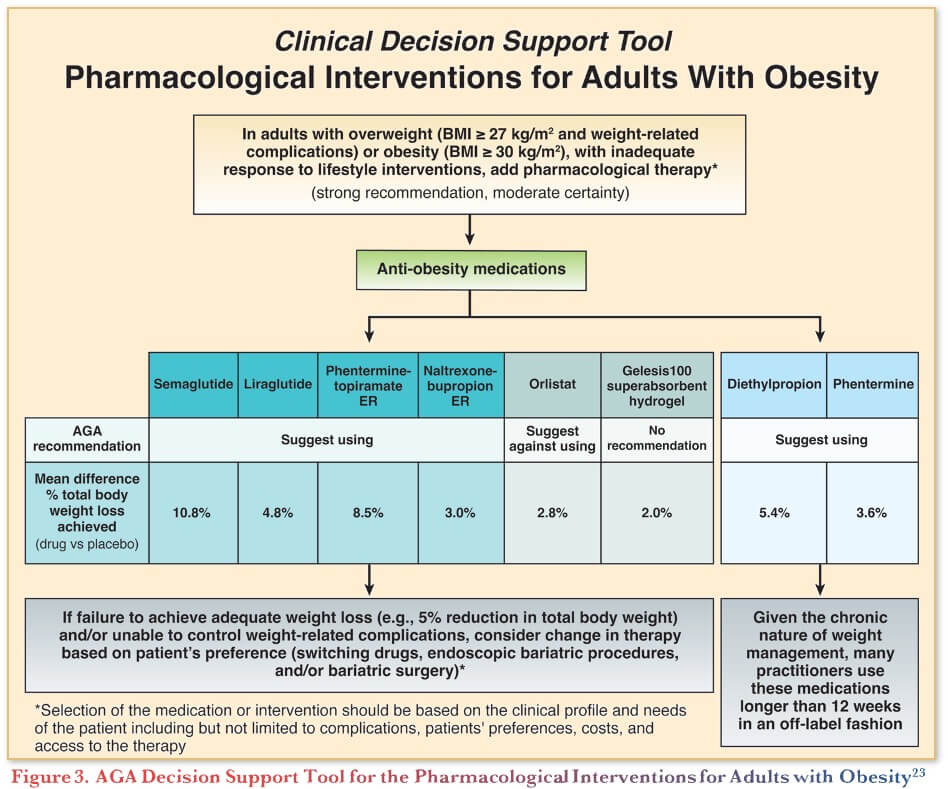
When considering the pharmacologic management of obesity, gastroenterologists can refer to the American Gastroenterological Association (AGA) Clinical Practice Guideline and Clinical Decision Support Tool on Pharmacological Interventions for Adults with Obesity (Figure 3).22,23
The field of pharmacotherapy in obesity has expanded substantially showing multiple options with good efficacy. Furthermore, many of these medications have pre-clinical data in IBD. For example, computational analysis with topiramate comparing gene expression profiles, showed that the genes turned on were similar to prednisone, suggesting a potential anti-inflammatory effect.24
There are also emerging data with respect to glucagon-like peptide 1 (GLP-1) agonist /dipeptidyl peptidase 4 (DPP-4) inhibitor-based therapies and disease course of IBD. In a study of 3,751 patients with IBD and diabetes mellitus from Danish registries compared 982 patients treated with GLP-1 receptor agonists/DPP-4 inhibitors vs. 2,769 patients treated with other anti-diabetic agents. The results showed that for the composite outcome (need for corticosteroids, anti-TNFs, IBD-related hospitalization, or IBD-related surgery), GLP-1 receptor agonists/DPP-4 inhibitors were associated with a 48% lower risk, suggesting potential to improve disease course in IBD.25 Given this evidence, further study is underway to investigate the impact of weight loss agents in IBD.
Conclusions
To summarize, obesity is common in patients with IBD, and may contribute to increased risk of developing CD and adversely impact disease course and outcomes. Obesity can lead to inferior response to biologic therapy, potentially by promoting rapid drug clearance regardless of dose, thus treating obesity may augment treatment response to biologics and improve patient outcomes in IBD.
Clinical Case
Maia—28-year-old female engineer
- 9-year history of ileocolonic Crohn’s disease, well controlled on azathioprine
- For two months she has had:
- Up to four to six BMs per day
- Abdominal cramps
- More recent decrease in appetite
- Maia not initially concerned, as she had gained 12 kg over 18 months, which she attributes to lack of exercise, and working from home with easy access to snacks during COVID pandemic
- Baseline weight 55 kg
- Current weight 67 kg—wants to get back to baseline
- Height 1.55 m
- Current BMI of 27.9 kg/m2
- Azathioprine (AZA) dose constant at 100 mg daily
- Her investigations reveal:
- WBC: 3.2 x 109/L
- Hb: 109 g/L
- CRP: 11 mg/L
- Alb: 38 g/L
- Fecal calprotectin: 1342 mcg/g
- Stool C and S negative
- difficile negative
- Colonoscopy reveals absence of deep ulcers, but aphthae in ileum and right colon, with surrounding erythema and edema
- Rest of colon appears unaffected
- SES-CD score = 7
Commentary
- In terms of continuing AZA, the expert panel would not continue the same dose, instead switching treatment or increasing the dosage and monitoring CBC
- Measurement of thiopurine methyltransferase (TPMT) and/or 6-mercaptopurine (6-MP) metabolites may be relevant as she is already mildly leukopenic
- Given thiopurines are slow acting, adjusting the dose may not be sufficient for managing her disease
- In terms of alternate treatment options, considering her comorbidities and weight gain, mild to moderate right-sided disease, budesonide is also a good option
Case Evolution
- After discussion with patient, you increase AZA to 150 mg and trial prednisone as she is not keen to start a biologic agent
- At 8-week review, stool frequency and consistency improved, and abdominal pain resolved
- However, she has developed lymphopenia
- Weight increased to 72 kg
- BMI 30.0 kg/m2
- A year passes—Maia returns for follow up
- She intentionally lost some weight
- Now weighs 69 kg
- BMI 28.7 kg/m2
- Lymphopenia long resolved, but…
- CRP 11 mg/L
- Fecal calprotectin now 5874 mcg/g
- Repeat colonoscopy reveals:
- Deep ulcerations in ileum and right colon
- Surrounding erythema and edema
- Aphthae in transverse colon
- Relative left colonic sparing
- SES-CD score of 16
- Prior biologic work up unremarkable
- She has received appropriate vaccinations
Commentary
In terms of which biologic to choose:
- Given she is not totally open to biologics, the expert panel would aim for less frequent administration
- For deep ulcers, data suggests anti-TNF is most effective in ileocolonic CD
- Weight-based dosing may be more appropriate, but unclear if obesity impacts the pharmacokinetics, or if they are less likely to response whether IV or SC, rather it may be due to inflammation modifying treatment response
- If the patient was older with higher BMI, they would be more concerned about MTX use
Case Evolution
- You decide to initiate IFX treatment
- Given history of lymphopenia, you do not restart azathioprine
- Instead, you start 15 mg oral MTX weekly with 5 mg folic acid per week
- She absolutely refuses another course of prednisone
Commentary
- Dose optimization of IFX may overcome any issues with volume distribution
- Proactive TDM is a contentious topic, observational studies support its use, but trials using proactive TDM (e.g., TAXIT) have shown mixed results in terms of clinical benefits
- No benefit of proactive TDM clearly demonstrated in trials, and has impact on costs and healthcare resource utilization so do not use it
- Evidence suggests combination therapy is more effective with IFX however, in patients hesitant to take biologics, it can be difficult to get them to agree to take 2 medications
- The expert panel would also consider the risk of pregnancy with respect to her starting MTX and recommend contraception
- In practice, there is a small proportion of patients that have disproportionate weight gain with biologic treatment, and this appears to be similar across biologic agents
- They would also discuss dietary and lifestyle factors that may be beneficial
Case Evolution
- Maia receives standard three-dose induction regimen of IFX, with a post-induction clinical response, but…
- IFX level pre-4th dose (week 14) is 2.4 mcg/mL
- You continue 5 mg/kg but optimize dosing to every 6 weeks
- At six-month follow-up she expresses concern about further weight gain of 6 kg which she attributes to IFX
- Current weight 75 kg
- BMI 31.2 kg/m2
- Despite prior dose optimization, IFX level now undetectable with low level antibodies
- Bowel ultrasound demonstrates:
- Ongoing activity in ileum and right colon with creeping fat
- Moderate hepatic steatosis
Commentary
- In terms of next steps, the expert panel would stop IFX
- They would consider initiating ADAL (combo with MTX) or UST monotherapy
Case Evolution
- After discussion, you switch to UST
- Maia is upset that you poisoned her liver with MTX
- She receives weight-based induction dose of UST 390 mg and subcutaneous doses 90 mg q8 weekly
- She declines ongoing MTX
- Six months after starting therapy, Maia has a clinical response:
- 1 formed BM/day
- CRP 3 mg/L
- Fecal calprotectin 537 mcg/g
- Her weight has not changed
- She wishes to start a weight loss ‘pill’ or consider surgery, as diet and exercise are not producing desired results
Commentary
- In practice, gastroenterologists do not tend to act differently based on obesity when choosing treatment, except for in obese patients that are refractory to treatment
- However, given the general benefits of weight loss, even if it does not help the patient’s IBD directly, it is something they should think about
- The bigger issue is whether some factor in obesity makes patients more resistant to treatment, and thus whether helping patients lose weight will impact their IBD outcomes
- They would also consider prescribing anti-obesity medications, as it could help
Case Evolution
- You are fortunate that you are attending Mentoring in IBD and eagerly await the expert opinions of our guest speaker and the panel discussion…
Commentary
- Obesity is associated with other metabolic issues, and this has not been adjusted for in the studies
- For example, metabolic syndrome will also impact outcomes in IBD
- Thus, it is important to look at the full picture, such as obesity in combination with diabetes, smoking, etc., which may present a complex interplay, and the cumulative impact is not known
- Integrated treatment models with obesity care will lead to an improvement in long-term IBD management
References
-
Ng M, Fleming T, Robinson M, et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2014;384:766–81.
-
Molodecky NA, Soon IS, Rabi DM. Increasing incidence and prevalence of the inflammatory bowel diseases with time, based on systematic review. Gastroenterology. 2012;142(1):46–54.
-
Seminerio JL, Koutroubakis IE, Ramos-Rivers C, et al. Impact of obesity on the management and clinical course of patients with inflammatory bowel disease. Inflamm Bowel Dis. 2015;21:2857–63.
-
Long MD, Crandall WV, Leibowitz IH, et al. Prevalence and epidemiology of overweight and obesity in children with inflammatory bowel disease. Inflamm Bowel Dis. 2011;17(10):2162–8.
-
Bhagavathula AS, Clark CCT, Rahmani J, et al. Impact of body mass index on the development of inflammatory bowel disease: A systematic review and dose-response analysis of 15.6 million participants. Healthcare. 2021;9(1):35; https://doi.org/10.3390/healthcare9010035.
-
Singh S, Dulai PS, Zarrinpar A, et al. Obesity in IBD: epidemiology, pathogenesis, disease course and treatment outcomes. Nat Rev Gastroenterol Hepatol. 2017;14(2):110–21.
-
Bapat SP, Whitty C, Mowery CT, et al. Obesity alters pathology and treatment response in inflammatory disease. Nature. 2022;604(7905):337–42.
-
Jain A, Nguyen N, Proudfoot JA, et al. Impact of obesity on disease activity and patient-reported outcomes measurement information system (PROMIS) in inflammatory bowel diseases. Am J Gastroenterol. 2019;114(4):630–9.
-
Johnson AM, Harmsen WS, Aniwan S, et al. Prevalence and impact of obesity on disease-specific outcomes in a population-based cohort of patients with ulcerative colitis. J Crohn’s Colitis. 2021;15(11):1816–23.
-
Erhayiem B, Dhingsa R, Hawkey CJ, et al. Ratio of visceral to subcutaneous fat area is a biomarker of complicated Crohn’s disease. Clin Gastroenterol Hepatol. 2011;9(8):684–7.
-
Uko V, Vortia E, Achkar J-P, et al. Impact of abdominal visceral adipose tissue on disease outcome in pediatric Crohn’s disease. Inflamm Bowel Dis. 2014;20(12):2286–91.
-
Rosario M, Dirks NL, Gastonguay MR, et al. Population pharmacokinetics-pharmacodynamics of vedolizumab in patients with ulcerative colitis and Crohn’s disease. Aliment Pharmacol Ther. 2015;42:188–202.
-
Ordás I, Mould DR, Feagan BG, et al. Anti-TNF monoclonal antibodies in inflammatory bowel disease: pharmacokinetics-based dosing paradigms. Clin Pharmacol Ther. 2012;91(4):635–46.
-
Kurnool S, Nguyen NH, Proudfoot J, et al. High body mass index is associated with increased risk of treatment failure and surgery in biologic-treated patients with ulcerative colitis. Aliment Pharmacol Ther. 2018;47(11):1472–9.
-
Singh S, Facciorusso A, Singh AG, et al. Obesity and response to anti-tumor necrosis factor-α agents in patients with select immune-mediated inflammatory diseases: A systematic review and meta-analysis. PLoS One. 2018;13(5):e0195123.
-
Singh S, Proudfoot J, Xu R, et al. Obesity and response to infliximab in patients with inflammatory bowel diseases: Pooled analysis of individual participant data from clinical trials. Am J Gastroenterol. 2018;113(6):883–9.
-
Gu P, Luo J, Kim J, et al. Effect of Obesity on Risk of Hospitalization, Surgery, and Serious Infection in Biologic-Treated Patients With Inflammatory Bowel Diseases: A CA-IBD Cohort Study. Am J Gastroenterol. 2022 Oct 1;117(10):1639–
-
Singh S, Picardo S, Seow CH. Management of inflammatory bowel diseases in special populations: Obese, old or obstetric. Clin Gastroenterol Hepatol. 2020;18(6):1367–47.
-
Di Minno MND, Peluso R, Lervolino S, et al. Weight loss and achievement of minimal disease activity in patients with psoriatic arthritis starting treatment with tumour necrosis factor α blockers. Ann Rheum Dis. 2014;73:1157–62.
-
Sparks JA, Halperin F, Karlson JC et al. Impact of bariatric surgery on patients with rheumatoid arthritis. Arthritis Care Res. 2015;67(12):1619–26.
-
Garg R, Mohan BP, Ponnada S, et al. Safety and efficacy of bariatric surgery in inflammatory bowel disease patients: a systematic review and meta-analysis. Obes Surg. 2020;30(10):3872–83.
-
Grunvald E, Shah R, Hernaez R, et al. AGA Clinical Practice Guideline on Pharmacological Interventions for Adults With Obesity. 2022;163(5):1198–225.
-
AGA Guideline. Clinical Decision Support Tool: Pharmacological Interventions for Adults with Obesity. 2022;163(5):1226.
-
Dudley JT, Sirota M, Shenoy M, et al. Computational repositioning of the anticonvulsant topiramate for inflammatory bowel disease. Sci Transl Med. 2011;3(96):96ra76.
-
Villumsen M, Schelde AB, Jimenez-Solem E, et al. GLP-1 based therapies and disease course of inflammatory bowel disease. EClinicalMedicine. 2021;37:100979.
Editor-in-Chief
John K. Marshall, MD MSc FRCPC AGAF, Director, Division of Gastroenterology, Professor, Department of Medicine, McMaster University, Hamilton, ON
Contributing Author
Siddharth Singh, MD MS, Director, UCSD IBD Center, Associate Professor of Medicine, Division of Gastroenterology and Division of Biomedical Informatics, University of California, San Diego, La Jolla, CA, USA
Mentoring in IBD Curriculum Steering Committee
Alain Bitton, MD FRCPC, McGill University, Montreal, QC
Karen I. Kroeker, MD MSc FRCPC, University of Alberta, Edmonton, AB
Cynthia Seow, MBBS (Hons) MSc FRACP, University of Calgary, Calgary, AB
Jennifer Stretton, ACNP MN BScN, St. Joseph’s Healthcare, Hamilton, ON
Eytan Wine, MD PhD FRCPC, University of Alberta, Edmonton, AB
IBD Dialogue 2023·Volume 19 is made possible by unrestricted educational grants from…
![]()
![]()
![]()

![]()

![]()
![]()
![]()
Published by Catrile & Associates Ltd., 167 Floyd Avenue, East York, ON M4J 2H9
(c) Catrile & Associates Ltd., 2023. All rights reserved. None of the contents may be reproduced in any form without prior written permission from the publisher. The opinions expressed in this paper are those of the authors and do not necessarily reflect the opinions or recommendations of the sponsors, the grantor, or the publisher.